

Restricted upper airway dimensions in patients with dentofacial deformity from juvenile idiopathic arthritis
- PMID: 35477405
- PMCID: PMC9044879
- DOI: 10.1186/s12969-022-00691-w
Restricted upper airway dimensions in patients with dentofacial deformity from juvenile idiopathic arthritis
Abstract
Background: This retrospective, cross-sectional study aimed to assess the pharyngeal airway dimensions of patients with juvenile idiopathic arthritis (JIA) and moderate/severe JIA-related dentofacial deformity (mandibular retrognathia/micrognathia), and compare the results with JIA patients with a normal mandibular appearance and a group of non-JIA patients.
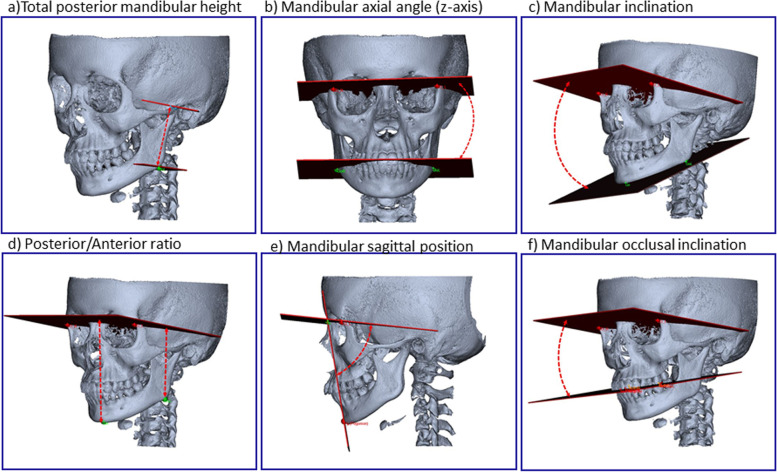
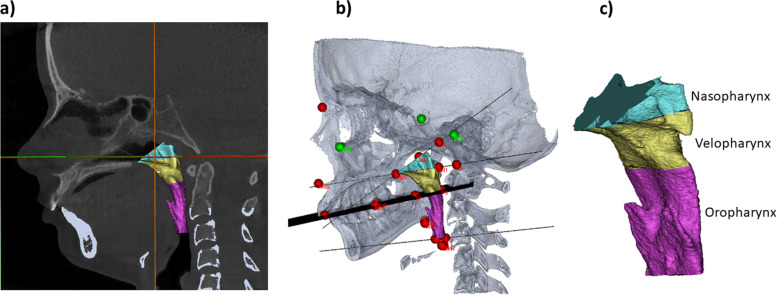
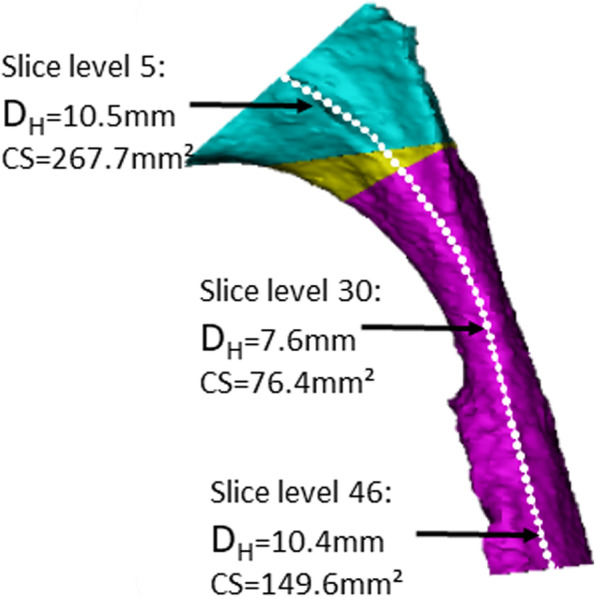
Methods: Seventy-eight patients were retrospectively included in a 1:1:1 manner as specified below. All patients had previously been treated at the Section of Orthodontics, Aarhus University, Denmark. All had a pretreatment cone beam computed tomography (CBCT). Group 1 (JIA+); 26 JIA patients with severe arthritis-related dentofacial deformity and mandibular retrognathia/micrognathia. Group 2 (JIA-); 26 JIA patients with normal mandibular morphology/position. Group 3 (Controls); 26 non-JIA subjects. Dentofacial morphology and upper airway dimensions, excluding the nasal cavity, were assessed in a validated three-dimensional (3D) fashion. Assessment of dentofacial deformity comprised six morphometric measures. Assessment of airway dimensions comprised nine measures.
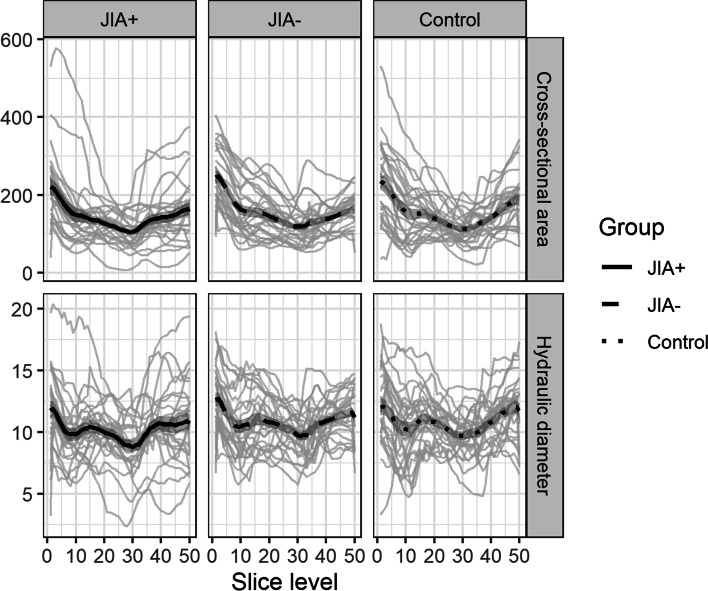
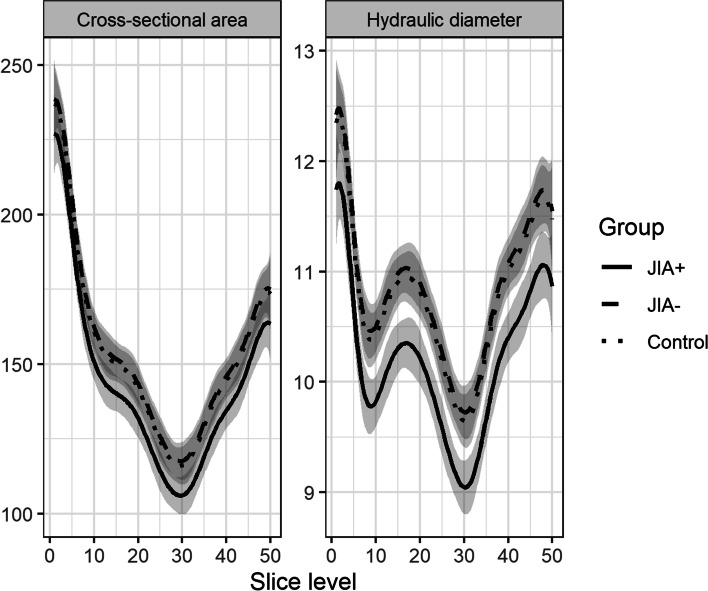
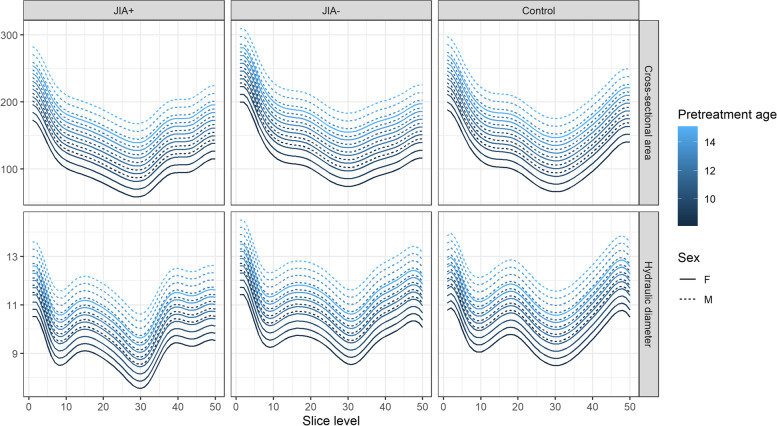
Results: Five morphometric measures of dentofacial deformity were significantly deviating in the JIA+ group compared with the JIA- and control groups: Posterior mandibular height, anterior facial height, mandibular inclination, mandibular occlusal inclination, and mandibular sagittal position. Five of the airway measurements showed significant inter-group differences: JIA+ had a significantly smaller nasopharyngeal airway dimension (ad2-PNS), a smaller velopharyngeal volume, a smaller minimal cross-sectional area and a smaller minimal hydraulic diameter than JIA- and controls. No significant differences in upper airway dimensions were seen between JIA- and controls.
Conclusion: JIA patients with severe arthritis-related dentofacial deformity and mandibular micrognathia had significantly restricted upper airway dimensions compared with JIA patients without dentofacial deformity and controls. The restrictions of upper airway dimension seen in the JIA+ group herein were previously associated with sleep-disordered breathing in the non-JIA background population. Further studies are needed to elucidate the role of dentofacial deformity and restricted airways in the development of sleep-disordered breathing in JIA.
© 2022. The Author(s).
Conflict of interest statement
No competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
