

Genetic insight into Birt-Hogg-Dubé syndrome in Indian patients reveals novel mutations at FLCN
- PMID: 35477461
- PMCID: PMC9044636
- DOI: 10.1186/s13023-022-02326-5
Genetic insight into Birt-Hogg-Dubé syndrome in Indian patients reveals novel mutations at FLCN
Abstract
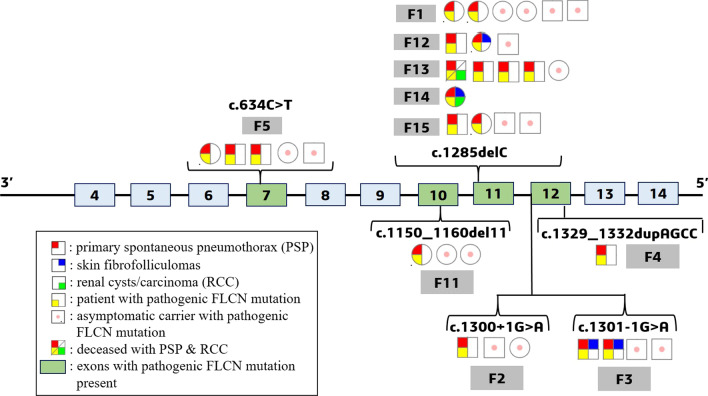
Background: Birt-Hogg-Dubé syndrome (BHDS) is a rare monogenic condition mostly associated with germline mutations at FLCN. It is characterized by either one or more manifestations of primary spontaneous pneumothorax (PSP), skin fibrofolliculomas and renal carcinoma (chromophobe). Here, we comprehensively studied the mutational background of 31 clinically diagnosed BHDS patients and their 74 asymptomatic related members from 15 Indian families.
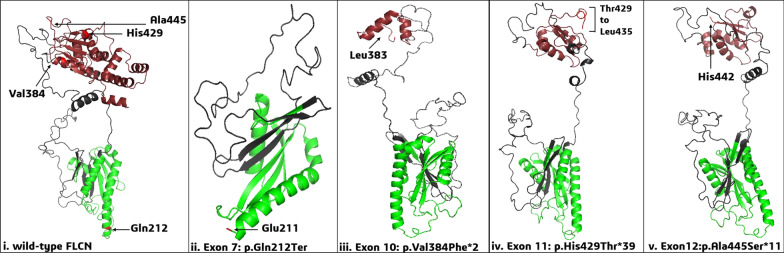
Results: Targeted amplicon next-generation sequencing (NGS) and Sanger sequencing of FLCN in patients and asymptomatic members revealed a total of 76 variants. Among these variants, six different types of pathogenic FLCN mutations were detected in 26 patients and some asymptomatic family members. Two of the variants were novel mutations: an 11-nucleotide deletion (c.1150_1160delGTCCAGTCAGC) and a splice acceptor mutation (c.1301-1G > A). Two variants were Clinvar reported pathogenic mutations: a stop-gain (c.634C > T) and a 4-nucleotide duplication (c.1329_1332dupAGCC). Two known variants were: hotspot deletion (c.1285delC) and a splice donor mutation (c.1300 + 1G > A). FLCN mutations could not be detected in patients and asymptomatic members from 5 families. All these mutations greatly affected the protein stability and FLCN-FNIP2 interaction as observed by molecular docking method. Family-based association study inferred pathogenic FLCN mutations are significantly associated with BHDS.
Conclusion: Six pathogenic FLCN mutations were detected in patients from 10 families out of 15 families in the cohort. Therefore, genetic screening is necessary to validate the clinical diagnosis. The pathogenic mutations at FLCN affects the protein-protein interaction, which plays key roles in various metabolic pathways. Since, pathogenic mutations could not be detected in exonic regions of FLCN in 5 families, whole genome sequencing is necessary to detect all mutations at FLCN and/or any undescribed gene/s that may also be implicated in BHDS.
Keywords: BHDS; FLCN mutations; Family-based association; Indian patients; Molecular docking; Primary spontaneous pneumothorax.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Birt AR, Hogg GR, Dubé WJ. Hereditary Multiple Fibrofolliculomas With Trichodiscomas and Acrochordons. Arch Dermatol. 1977;113:1674. - PubMed
-
- Zbar B, Alvord WG, Glenn G, Turner M, Pavlovich CP, Schmidt L, et al. Risk of renal and colonic neoplasms and spontaneous pneumothorax pneurnothorax in the Birt-Hogg-Dubé syndrome. Cancer Epidemiol Biomarkers Prev. 2002;11:393–400. - PubMed
-
- Nickerson ML, Warren MB, Toro JR, Matrosova V, Glenn G, Turner ML, et al. Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt–Hogg–Dubé syndrome. Cancer Cell. 2002;2:157–164. - PubMed
-
- Abolnik IZ, Lossos IS, Zlotogora J, Brauer R. On the inheritance of primary spontaneous pneumothorax. Am J Med Genet. 1991;40:155–158. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
