

Small fiber involvement is independent from clinical pain in late-onset Pompe disease
- PMID: 35477515
- PMCID: PMC9044713
- DOI: 10.1186/s13023-022-02327-4
Small fiber involvement is independent from clinical pain in late-onset Pompe disease
Abstract
Background: Pain occurs in the majority of patients with late onset Pompe disease (LOPD) and is associated with a reduced quality of life. The aim of this study was to analyse the pain characteristics and its relation to a small nerve fiber involvement in LOPD patients.
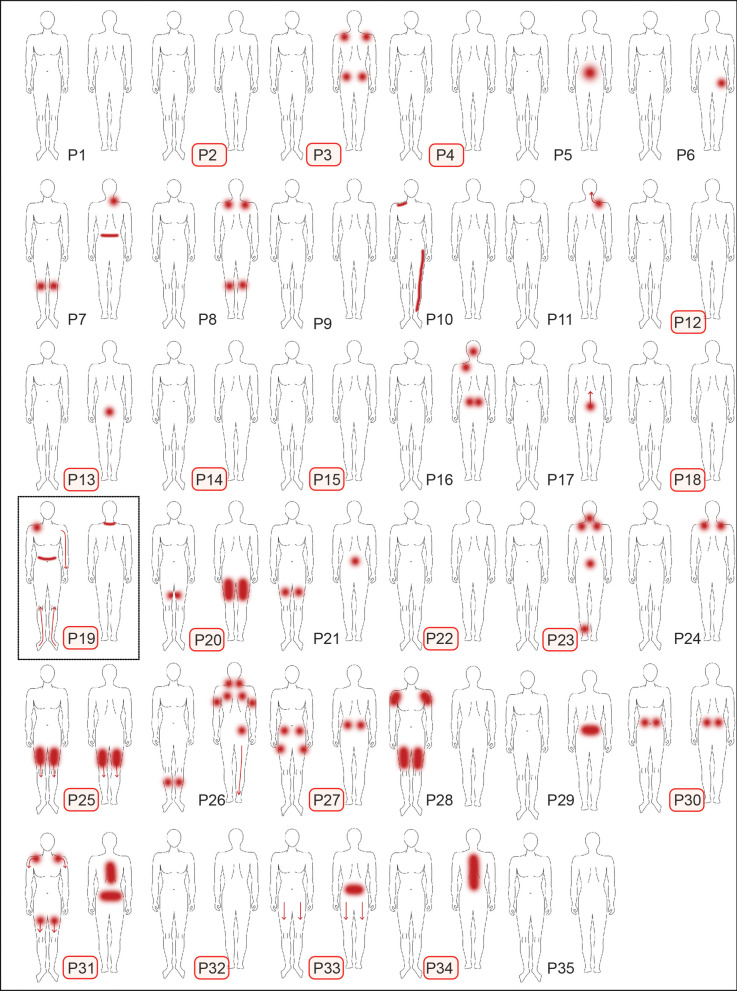
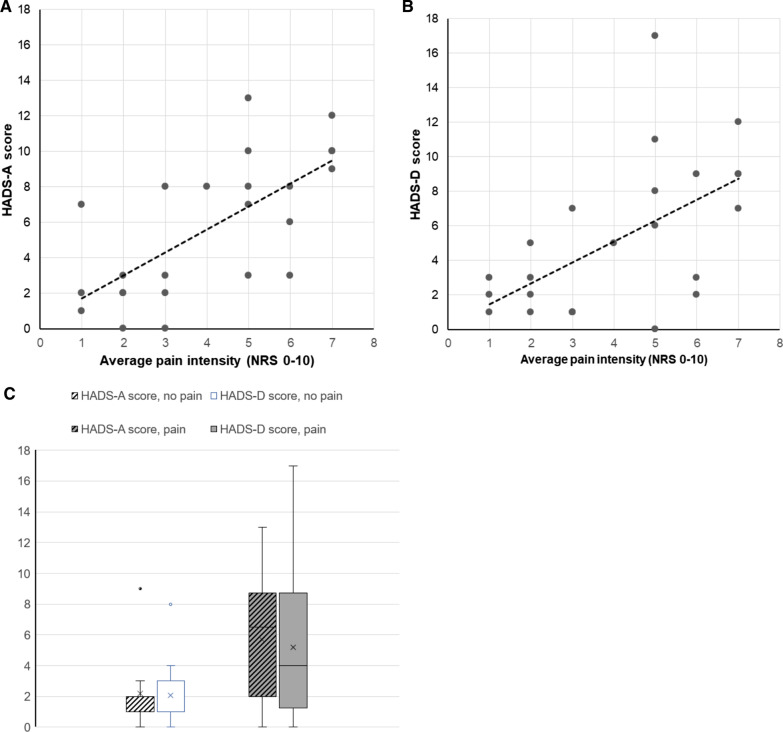
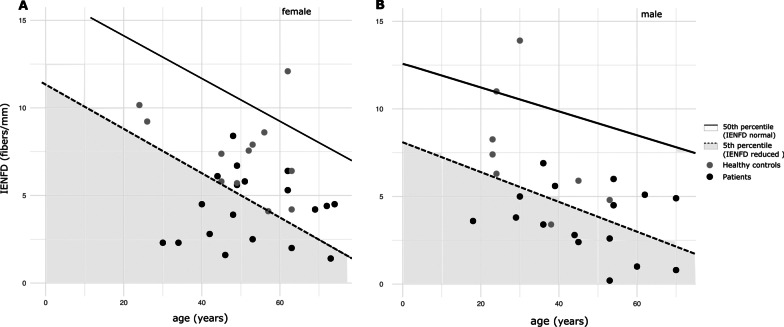
Methods: In 35 patients with LOPD under enzyme replacement therapy without clinical signs of polyneuropathy (19 females; 51 ± 15 years), pain characteristics as well as depressive and anxiety symptoms were assessed using the PainDetect questionnaire (PDQ) and the hospital anxiety and depression scale (HADS), respectively. Distal skin biopsies were analysed for intraepidermal nerve fiber density (IENFD) and compared to age- and gender-matched reference data. Skin biopsies from 20 healthy subjects served as controls to assure validity of the morphometric analysis.
Results: Pain was reported in 69% of the patients with an average intensity of 4.1 ± 1.1 on the numeric rating scale (NRS; anchors: 0-10). According to PDQ, neuropathic pain was likely in one patient, possible in 29%, and unlikely in 67%. Relevant depression and anxiety symptoms occurred in 31% and 23%, respectively, and correlated with pain intensity. Distal IENFD (3.98 ± 1.95 fibers/mm) was reduced in 57% of the patients. The degree of IENFD reduction did not correlate with the durations of symptoms to ERT or duration of ERT to biopsy.
Conclusions: Pain is a frequent symptom in treated LOPD on ERT, though a screening questionnaire seldom indicated neuropathic pain. The high frequency of small nerve fiber pathology in a treated LOPD cohort was found regardless of the presence of pain or comorbid risk factors for SFN and needs further exploration in terms of clinical context, exact mechanisms and when developing novel therapeutic options for LOPD.
Keywords: Intraepidermal nerve fiber density; Late onset Pompe disease; Pain; Skin biopsy; Small nerve fiber.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest in respect of the manuscript content.
Figures


References
-
- Montagnese F, Barca E, Musumeci O, Mondello S, Migliorato A, Ciranni A, Rodolico C, De Filippi P, Danesino C, Toscano A. Clinical and molecular aspects of 30 patients with late-onset Pompe disease (LOPD): unusual features and response to treatment. J Neurol. 2015;262:968–978. - PubMed
-
- Kroos MA, Pomponio RJ, Hagemans ML, Keulemans JL, Phipps M, DeRiso M, Palmer RE, Ausems MG, Van Beek NA, Van Diggelen OP, et al. Broad spectrum of Pompe disease in patients with the same c.-32–13T>G haplotype. Neurology. 2007;68:110–115. - PubMed
-
- Kroos M, Hoogeveen-Westerveld M, van der Ploeg A, Reuser AJ. The genotype-phenotype correlation in Pompe disease. Am J Med Genet C Semin Med Genet. 2012;160c:59–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
