

Pseudoaneurysm with a fistula to the right ventricle late after surgical repair of type A aortic dissection in a patient with systemic lupus erythematosus
- PMID: 35477534
- PMCID: PMC9044762
- DOI: 10.1186/s13019-022-01827-5
Pseudoaneurysm with a fistula to the right ventricle late after surgical repair of type A aortic dissection in a patient with systemic lupus erythematosus
Abstract
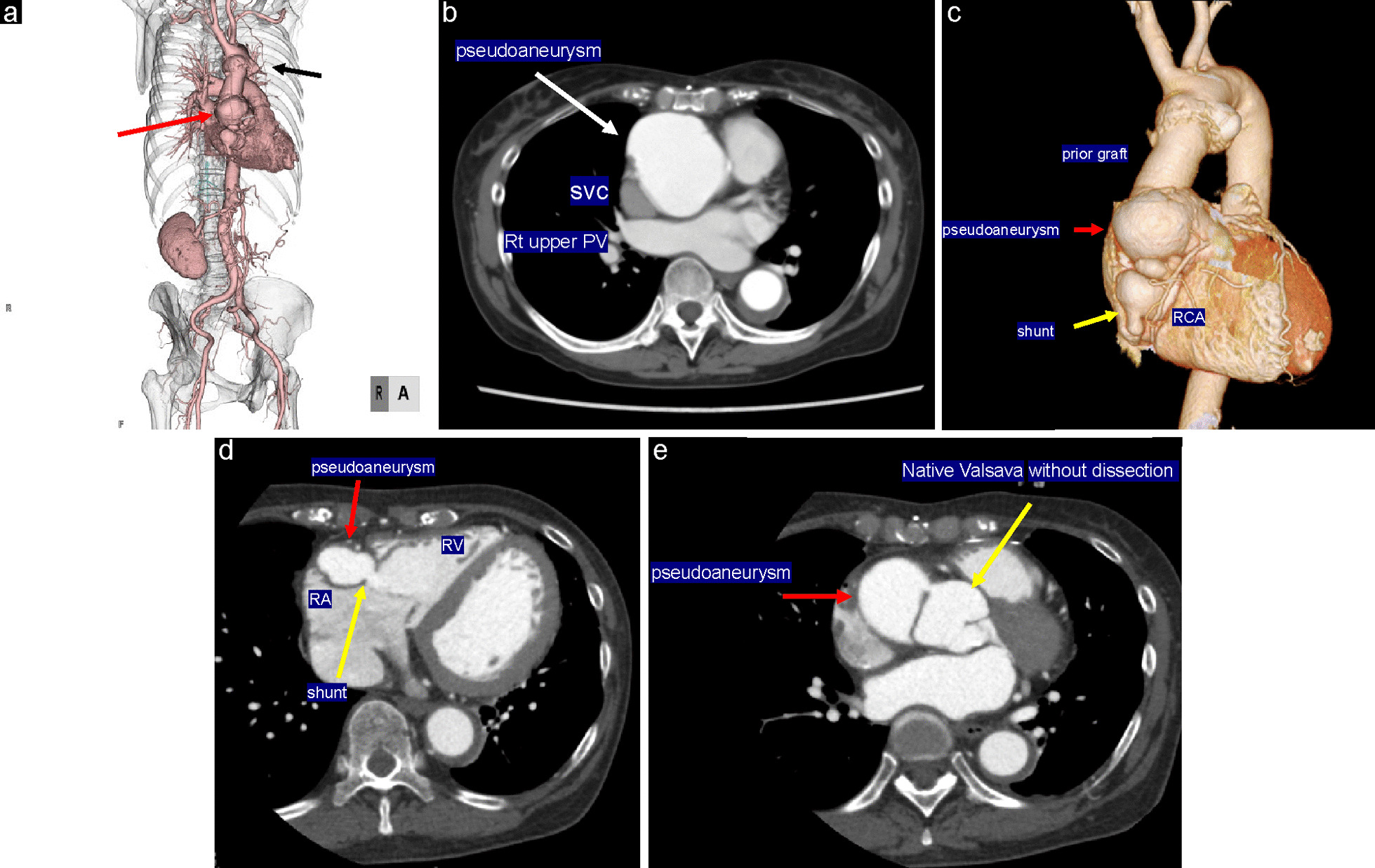
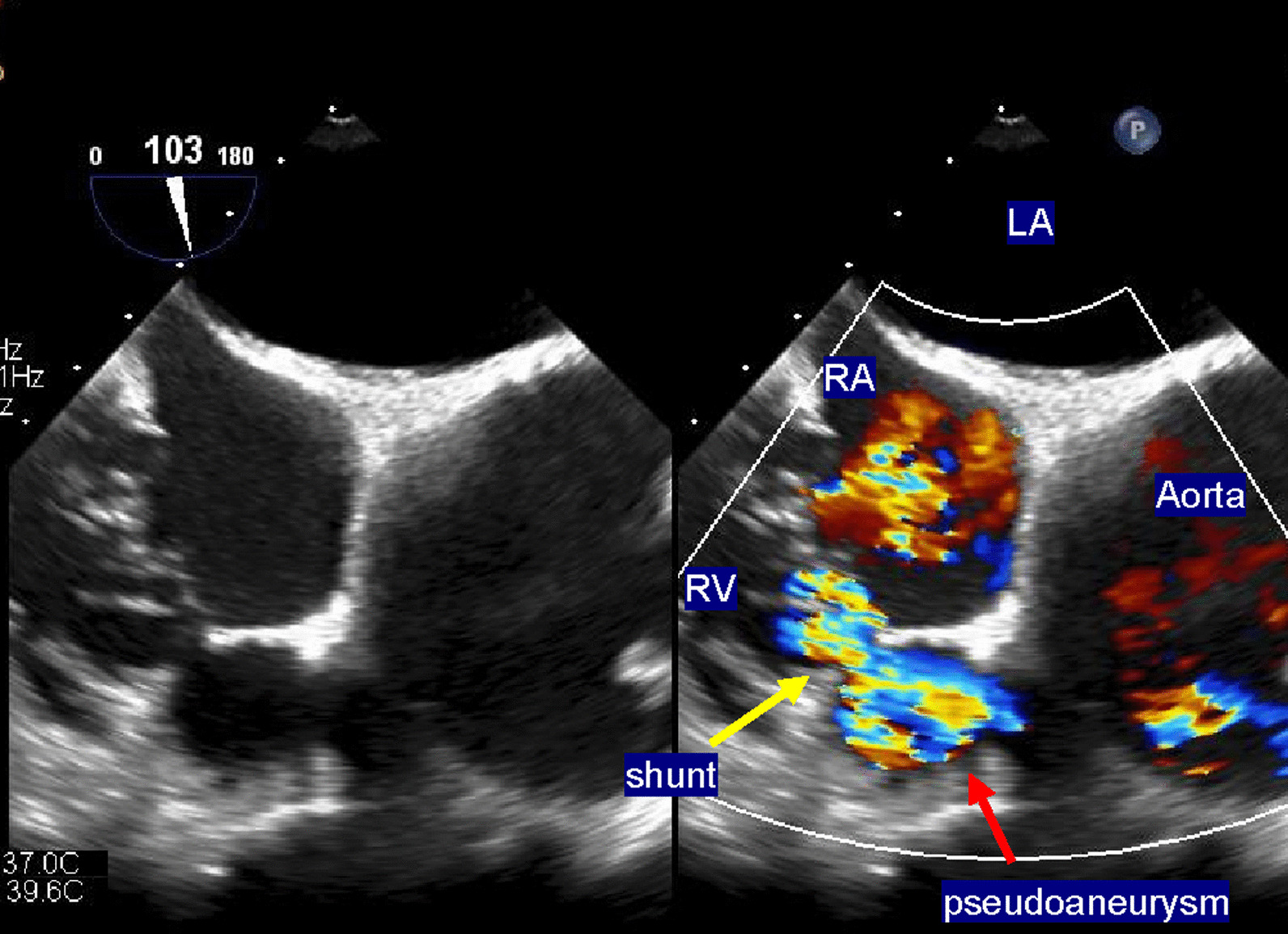
Background: Pseudoaneurysm with a shunt to the right ventricle after aortic repair for acute aortic dissection is an extremely rare and life-threatening condition. Surgical treatment is unavoidable, but surgery is complicated, and there are some pitfalls. This study describes the reoperation performed in a patient at a high surgical risk by clarifying the shunt site using multimodality imaging before surgery.
Case presentation: A 69-year-old woman with a history of systemic lupus erythematosus (SLE) and Sjogren's syndrome presented with a pseudoaneurysm 1 year after emergency surgery for acute type A aortic dissection. Eight years after the first surgery, she experienced sudden chest pain and presented to the emergency department. Her dyspnea worsened; therefore, echocardiography and three-dimensional computed tomography (3DCT) were performed, and a pseudoaneurysm and shunt to the right ventricle were identified. The medical team attempted to close the shunt with a percutaneous catheter but was unsuccessful, and she was referred to our department for surgical treatment. The pseudoaneurysm originating from the proximal side of the aorta was large (diameter = 55 mm), and echocardiography-gated 3DCT identified the shunt from the pseudoaneurysm to the right ventricle. First, extracorporeal circulation was initiated, and resternotomy was performed. We could not insert the left ventricular venting tube from the right side because of the pseudoaneurysm size. Instead, the tube was inserted from the left atrial appendage. We found a half-circumferential disengaged anastomosis around the proximal anastomosis, which formed the large pseudoaneurysm leading to a fistula in the right ventricle. We closed the fistula and performed a Bentall operation. The patient had a good postoperative course and was discharged on postoperative day 21. She continued treatment for SLE and Sjogren's syndrome, and her inflammatory reaction improved.
Conclusions: We performed a Bentall operation and fistula closure with resternotomy in a patient with type A aortic dissection with SLE and Sjogren's syndrome. Multimodal imaging is essential in defining the pseudoaneurysm and the fistula surrounding the anatomy while ensuring their resolution and guiding the approach for operation.
Keywords: Aortic dissection; Echocardiography-gated three-dimensional computed tomography; Fistula; Pseudoaneurysm; Sjogren’s syndrome; Systemic lupus erythematosus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
