

Open-aqueduct LOVA, LIAS, iNPH: a comparative clinical-radiological study exploring the "grey zone" between different forms of chronic adulthood hydrocephalus
- PMID: 35477816
- PMCID: PMC9233635
- DOI: 10.1007/s00701-022-05215-9
Open-aqueduct LOVA, LIAS, iNPH: a comparative clinical-radiological study exploring the "grey zone" between different forms of chronic adulthood hydrocephalus
Abstract
Purpose: The definition of chronic adult hydrocephalus encompasses different pathological entities with overlapping characteristics, including long-standing overt ventriculomegaly in adults (LOVA), late-onset idiopathic aqueductal stenosis (LIAS) and idiopathic normal pressure hydrocephalus (iNPH). The aim of our study was to identify preoperative clinical and radiological features peculiar of these diseases providing some pathophysiology inferences on these forms of hydrocephalus.
Methods: Clinical and radiological preoperative records, type of surgical treatment and clinical outcome of patients with chronic adult hydrocephalus who were surgically treated between 2013 and 2019 were retrospectively reviewed. Univariate and multivariate analyses were performed to evaluate the contribution of each variable to the differential diagnosis.
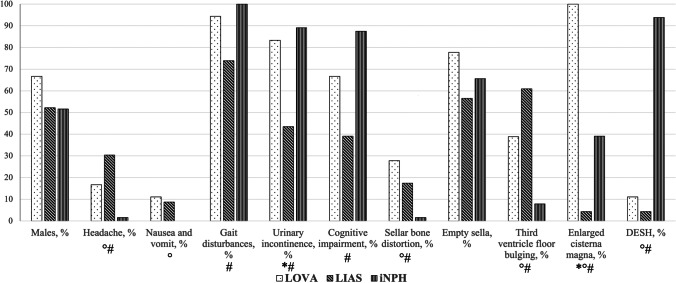
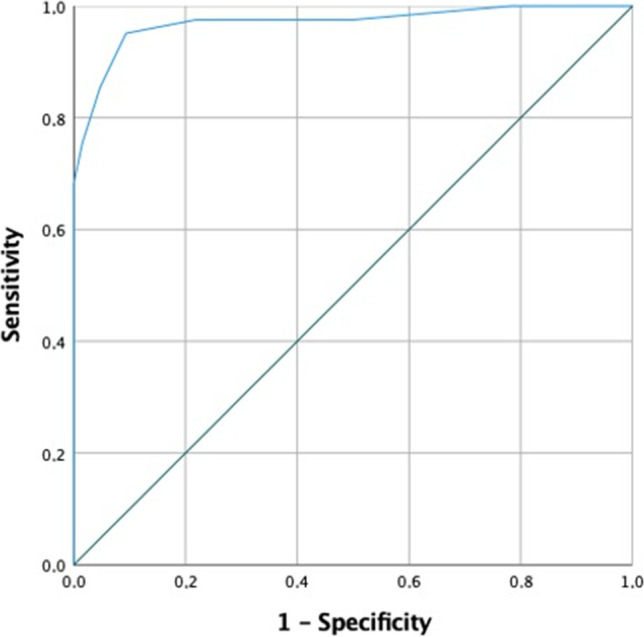
Results: In total, 105 patients were included: 18 with LOVA, 23 with LIAS and 64 with iNPH. On multivariate analysis, an enlarged cisterna magna and a more severe ventriculomegaly were associated with the diagnosis of LOVA, while an older age and DESH with iNPH. LIAS patients tend to have an higher prevalence of raised ICP symptoms. Based on that, a clinical and radiological scoring system was developed to distinguish between iNPH and no iNPH cases. A precise cut-off value with a sensitivity of 95.1% and a specificity of 90.6% was identified.
Conclusions: LOVA, LIAS and iNPH are different forms of chronic adulthood hydrocephalus and present different and peculiar clinical and radiological features, with an impact on the treatment and outcome prediction. The implementation of a clinical-radiological score for differential diagnosis may help the differentiation. Further studies are warranted.
Keywords: Differential diagnosis; Idiopathic normal pressure hydrocephalus (iNPH); Late-onset idiopathic aqueductal stenosis (LIAS); Longstanding overt ventriculomegaly in adults (LOVA); Score.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Boon AJ, Tans JT, Delwel EJ, Egeler-Peerdeman SM, Hanlo PW, Wurzer HA, Avezaat CJ, de Jong DA, Gooskens RH, Hermans J. Dutch normal-pressure hydrocephalus study: prediction of outcome after shunting by resistance to outflow of cerebrospinal fluid. J Neurosurg. 1997;87(5):687–693. doi: 10.3171/jns.1997.87.5.0687. - DOI - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
