

Circulating Autoantibodies Recognizing Immunodominant Epitopes From Human Apolipoprotein B Associate With Cardiometabolic Risk Factors, but Not With Atherosclerotic Disease
- PMID: 35479271
- PMCID: PMC9035541
- DOI: 10.3389/fcvm.2022.826729
Circulating Autoantibodies Recognizing Immunodominant Epitopes From Human Apolipoprotein B Associate With Cardiometabolic Risk Factors, but Not With Atherosclerotic Disease
Abstract
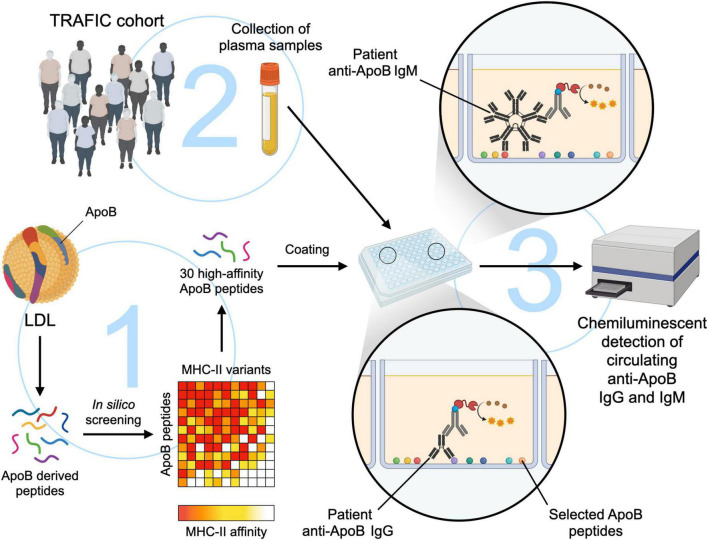
Rationale: Atherosclerosis is a chronic inflammatory disease of large arteries that involves an autoimmune response with autoreactive T cells and auto-antibodies recognizing Apolipoprotein B (ApoB), the core protein of low-density lipoprotein (LDL). Here, we aimed to establish a clinical association between circulating human ApoB auto-antibodies with atherosclerosis and its clinical risk factors using a novel assay to detect auto-antibodies against a pool of highly immunogenic ApoB-peptides.
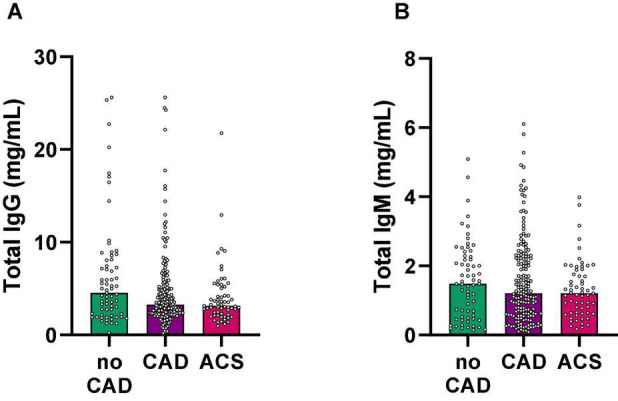
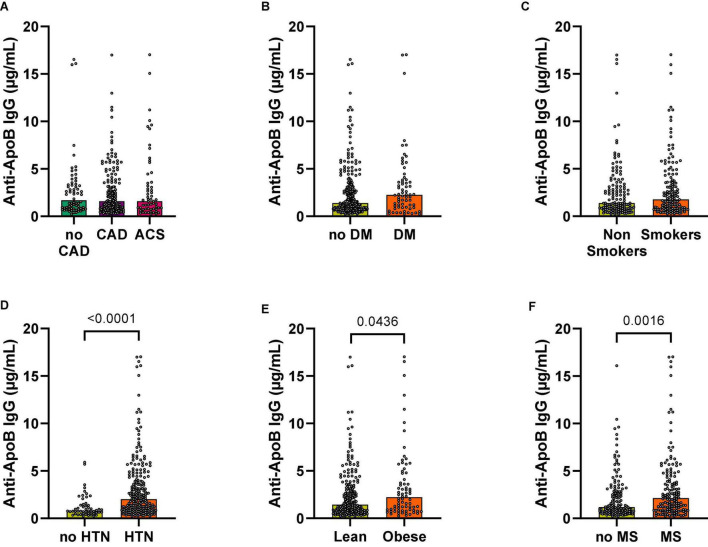
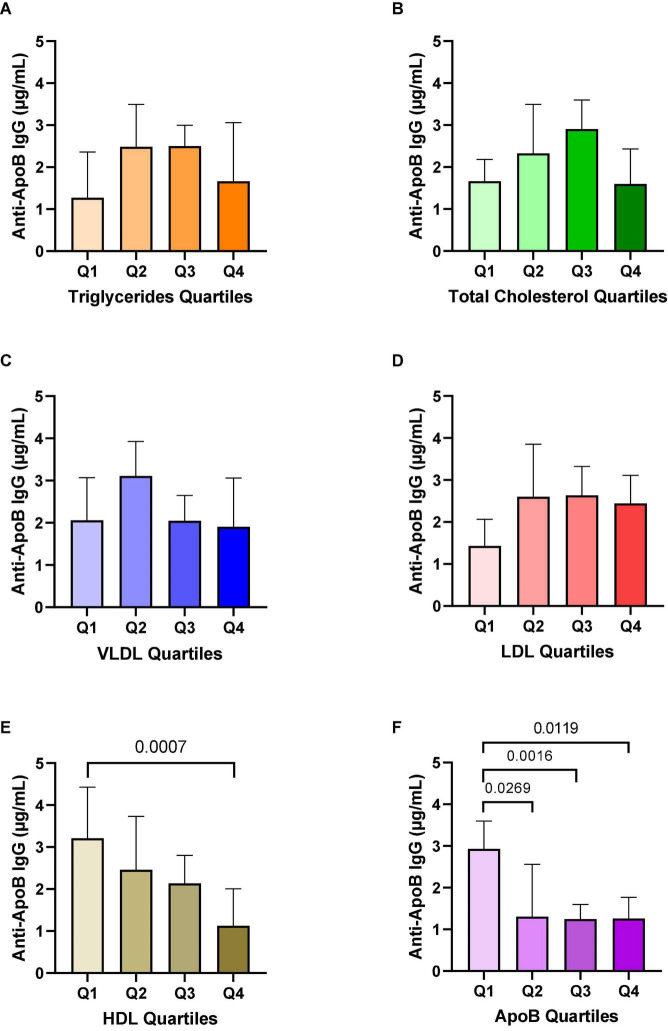
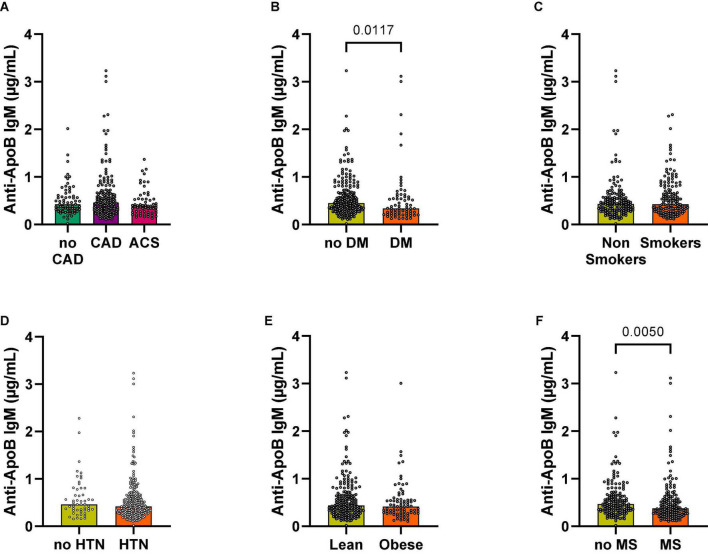
Methods and results: To detect polyclonal IgM- and IgG-antibodies recognizing ApoB, we developed a chemiluminescent sandwich ELISA with 30 ApoB peptides selected by an in silico assay for a high binding affinity to MHC-II, which cover more than 80% of known MHC-II variants in a Caucasian population. This pre-selection of immunogenic self-peptides accounted for the high variability of human MHC-II, which is fundamental to allow T cell dependent generation of IgG antibodies. We quantified levels of ApoB-autoantibodies in a clinical cohort of 307 patients that underwent coronary angiography. Plasma anti-ApoB IgG and IgM concentrations showed no differences across healthy individuals (n = 67), patients with coronary artery disease (n = 179), and patients with an acute coronary syndrome (n = 61). However, plasma levels of anti-ApoB IgG, which are considered pro-inflammatory, were significantly increased in patients with obesity (p = 0.044) and arterial hypertension (p < 0.0001). In addition, patients diagnosed with the metabolic syndrome showed significantly elevated Anti-ApoB IgG (p = 0.002). Even when normalized for total plasma IgG, anti-ApoB IgG remained highly upregulated in hypertensive patients (p < 0.0001). We observed no association with triglycerides, total cholesterol, VLDL, or LDL plasma levels. However, total and normalized anti-ApoB IgG levels negatively correlated with HDL. In contrast, total and normalized anti-ApoB IgM, that have been suggested as anti-inflammatory, were significantly lower in diabetic patients (p = 0.012) and in patients with the metabolic syndrome (p = 0.005).
Conclusion: Using a novel ELISA method to detect auto-antibodies against ApoB in humans, we show that anti-ApoB IgG associate with cardiovascular risk factors but not with the clinical appearance of atherosclerosis, suggesting that humoral immune responses against ApoB are shaped by cardiovascular risk factors but not disease status itself. This novel tool will be helpful to develop immune-based risk stratification for clinical atherosclerosis in the future.
Keywords: ApoB; atherosclerosis; auto-antibodies; cardiovascular disease; immunity.
Copyright © 2022 Marchini, Malchow, Caceres, El Rabih, Hansen, Mwinyella, Spiga, Piepenburg, Horstmann, Olawale, Li, Mitre, Gissler, Bugger, Zirlik, Heidt, Hilgendorf, Stachon, von zur Muehlen, Bode and Wolf.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous