

Case Reports
doi: 10.1016/j.radcr.2022.03.086.
eCollection 2022 Jun.
Dissective tandem stroke: an endovascular approach
Affiliations
- PMID: 35479967
- PMCID: PMC9035657
- DOI: 10.1016/j.radcr.2022.03.086
Item in Clipboard
Case Reports
Dissective tandem stroke: an endovascular approach
Radiol Case Rep.
.
Abstract
Ischemic stroke due to internal carotid artery occlusion is a potential devastating condition. More frequently the occlusions are embolic in nature, but sometimes they are caused by arterial dissection and their treatment is a challenge. We describe an illustrative case where a young patient with middle cerebral artery stroke caused by carotid artery dissection was submitted to endovascular treatment of mechanical thrombectomy and stenting, giving an excellent outcome. We believe that tandem approach is a treatment of choice in these cases.
© 2022 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
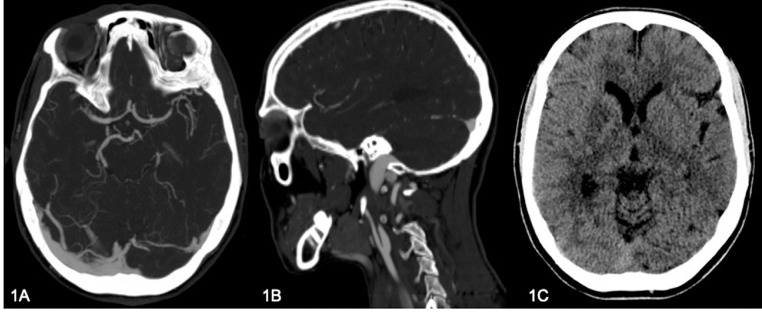
CT angiogram shows on axial plane (A) a middle cerebral arteries asymmetry for occlusion of right M1, while on sagittal plane (B) it shows dissective occlusion of right internal carotid artery (“flame sign”). (C) CT scan documenting a subtle hypodense area in the right lenticular region.

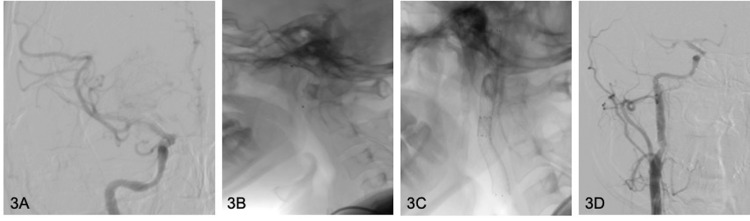
DSA study shows (A) dissective occlusion of right internal carotid artery with (B) stasis in venous phase and (C) ipsilateral middle cerebral artery (tandem) occlusion.
(A) Final DSA control documents TICI III revascularization of right middle cerebral artery. B shows positioning of the endovascular protection system Spider FX before stent releasing. (C, D) Correct opening and positioning of two overlapped carotid stents with consequent restored caliber of right internal carotid artery.

Axial DWI and ADC map images, acquired 1 month after the procedure, document malacic area in right caudate region, as result of ischemic insult.

Coronal MIP TOF sequence of same exam as Figure 4 documenting regular signal and caliber of intracranial arterial vessels.
References
-
- Chandra A., Suliman A., Angle N. Spontaneous dissection of the carotid and vertebral arteries: The 10-year UCSD experience. Ann. Vasc. Surg. 2007;21:178–185. - PubMed
-
- Schievink WI. Spontaneous dissection of the carotid and vertebral arteries. N Engl J Med. 2001;344:898–906. - PubMed
-
- Fusca M.R., Harrigan M.R. Cerebrovascular dissections—A review part I: Spontaneous dissections. Neurosurgery. 2011;68:242–257. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
