

Determining the frequency and level of task-sharing for hypertension management in LMICs: A systematic review and meta-analysis
- PMID: 35480075
- PMCID: PMC9035722
- DOI: 10.1016/j.eclinm.2022.101388
Determining the frequency and level of task-sharing for hypertension management in LMICs: A systematic review and meta-analysis
Abstract
Background: Low- and middle-income countries (LMICs) bear a disproportionately higher burden of Cardiovascular Disease (CVD). Team-based care approach adds capacity to improve blood pressure (BP) control. This updated review aimed to test team-based care efficacy at different levels of hypertension team-based care complexity.
Methods: We searched PubMed, Embase, Cochrane, and CINAHL for newer articles on task-sharing interventions to manage hypertension in LMICs. Levels of tasks complexity performed by healthcare workers added to the clinical team in hypertension control programs were categorized as administrative tasks (level 1), basic clinical tasks (level 2), and/or advanced clinical tasks (level 3). Meta-analysis using an inverse variance weighted random-effects model summarized trial-based evidence on the efficacy of team-based care on BP control, compared with usual care.
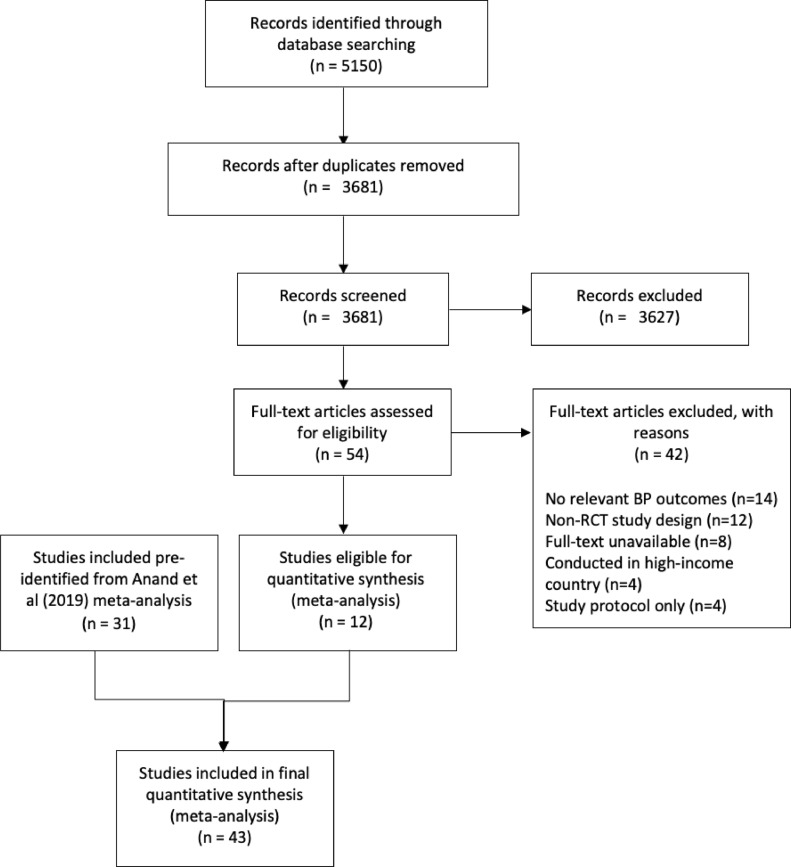
Findings: Forty-three RCT articles were included in the meta-analysis: 31 studies from the previous systematic review, 12 articles from the updated search. The pooled mean effect for team-based care was a -4.6 mm Hg (95% CI: -5.8, -3.4, I2 = 80.2%) decrease in systolic BP compared with usual care. We found similar comparative reduction among different levels of team-based care complexity, i.e., administrative and basic clinical tasks (-4.7 mm Hg, 95% CI: -6.8, -2.2; I2 = 79.8%); and advanced clinical tasks (-4.5 mmHg, 95%CI: -6.1, -3.3; I2 = 81%). Systolic BP was reduced most by team-based care involving pharmacists (-7.3 mm Hg, 95% CI: -9.2, -5.4; I2 = 67.2%); followed by nurses (-5.1 mm Hg, 95% CI: -8.0, -2.2; I2 = 72.7%), dieticians (-4.7 mmHg, 95%CI: -7.1, -2.3; I2 = 0.0%), then community health workers (-3.3 mm Hg, 95% CI: -4.8, -1.8; I2 = 77.3%).
Interpretation: Overall, team-based hypertension care interventions consistently contributed to lower systolic BP compared to usual care; the effect size varies by the clinical training of the healthcare team members.
Funding: Resolve To Save Lives (RTSL) Vital Strategies, Danielle Cazabon, Andrew E. Moran, Yvonne Commodore-Mensah receive salary support from Resolve to Save Lives, an initiative of Vital Strategies. Resolve to Save Lives is jointly supported by grants from Bloomberg Philanthropies, the Bill & Melinda Gates Foundation, and Gates Philanthropy Partners, which is funded with support from the Chan Zuckerberg Foundation.
Keywords: Hypertension; LMIC; Team-based care.
© 2022 The Authors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- World Health Organization . No Health Without a Workforce; Geneva: 2013. A Universal Truth.
-
- World Health Organization . workforce 2030; 2016. Global strategy on human resources for health.
-
- World Health Organization . WHO; Geneva: 2017. Task sharing to improve access to Family Planning/Contraception.
-
- World Health Organization . Geneva; 2008. Operations manual for delivery of HIV prevention, care and treatment at primary health centres in high-prevalence, resource-constrained settings: Edition 1 for fieldtesting and country adaptation. - PubMed
LinkOut - more resources
Full Text Sources
