

Development of a 5-Gene Signature to Evaluate Lung Adenocarcinoma Prognosis Based on the Features of Cancer Stem Cells
- PMID: 35480140
- PMCID: PMC9036162
- DOI: 10.1155/2022/4404406
Development of a 5-Gene Signature to Evaluate Lung Adenocarcinoma Prognosis Based on the Features of Cancer Stem Cells
Retraction in
-
Retracted: Development of a 5-Gene Signature to Evaluate Lung Adenocarcinoma Prognosis Based on the Features of Cancer Stem Cells.Biomed Res Int. 2024 Mar 20;2024:9867431. doi: 10.1155/2024/9867431. eCollection 2024. Biomed Res Int. 2024. PMID: 38550164 Free PMC article.
Abstract
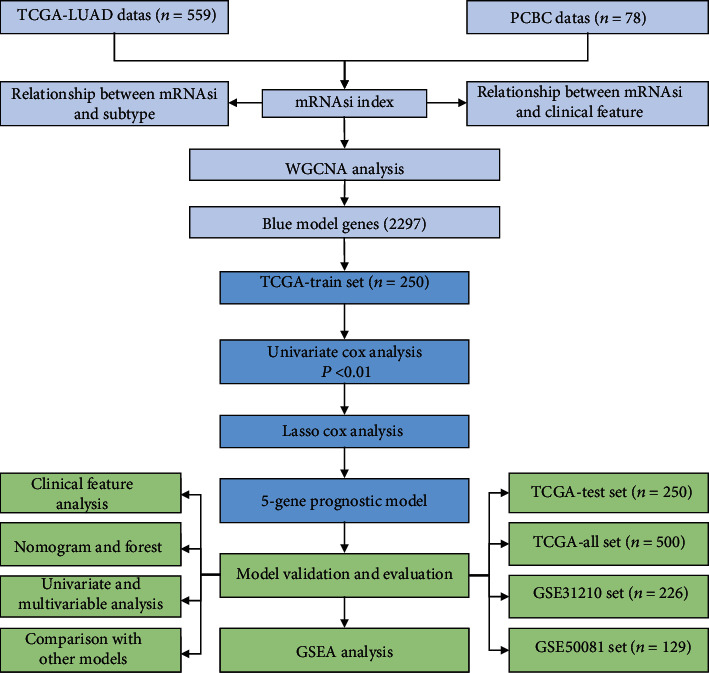
Cancer stem cells (CSCs) can induce recurrence and chemotherapy resistance of lung adenocarcinoma (LUAD). Reliable markers identified based on CSC characteristic of LUAD may improve patients' chemotherapy response and prognosis. OCLR was used to calculate mRNA expression-based stemness index (mRNAsi) of LUAD patients' data in TCGA. Association analysis of mRNAsi was performed with clinical features, somatic mutation, and tumor immunity. A prognostic prediction model was established with LASSO Cox regression. Kaplan-Meier Plotter (KM-plotter) and time-dependent ROC were applied to assess signature performance. For LUAD, univariate and multivariate Cox analysis was performed to identify independent prognostic factors. LUAD tissues showed a noticeably higher mRNAsi in than nontumor tissues, and it showed significant differences in T, N, M, AJCC stages, and smoking history. The most frequently mutated gene was TP53, with a higher mRNAsi relating to more frequent mutation of TP53. The mRNAsi was significantly negatively correlated with immune score, stromal score, and ESTIMATE score in LUAD. The blue module was associated with mRNAsi. The 5-gene signature was confirmed as an independent indicator of LUAD prognosis that could promote personalized treatment of LUAD and accurately predict overall survival (OS) of LUAD patients.
Copyright © 2022 Renping Wan et al.
Conflict of interest statement
The authors declare no conflict of interests.
Figures










References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
