

Evaluation of radio-immunotherapy sequence on immunological responses and clinical outcomes in patients with melanoma brain metastases (ELEKTRA)
- PMID: 35481285
- PMCID: PMC9037491
- DOI: 10.1080/2162402X.2022.2066609
Evaluation of radio-immunotherapy sequence on immunological responses and clinical outcomes in patients with melanoma brain metastases (ELEKTRA)
Abstract
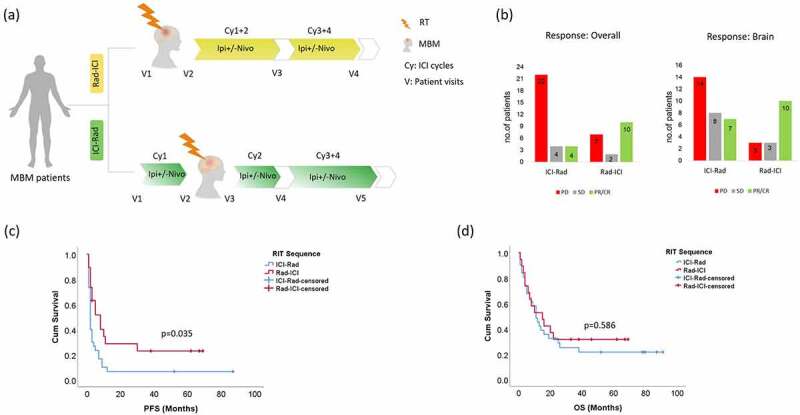
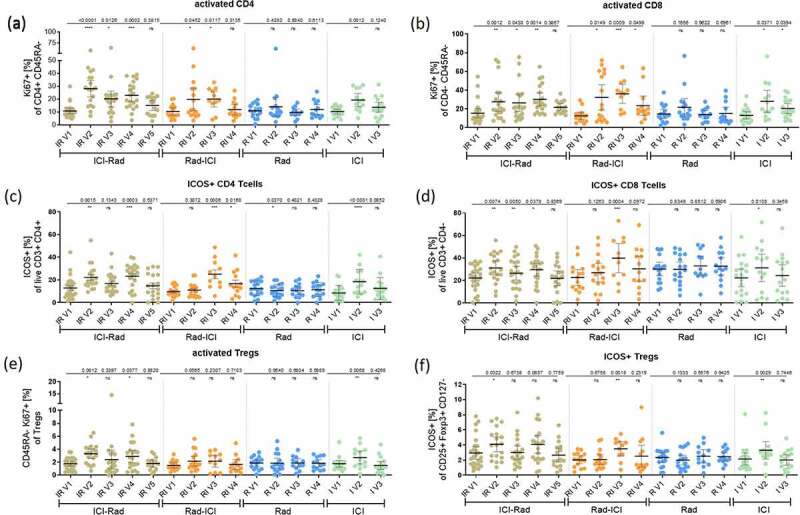
In patients with melanoma brain metastases (MBM), a combination of radiotherapy (RT) with immune checkpoint inhibitors (ICI) is routinely used. However, the best sequence of radio-immunotherapy (RIT) remains unclear. In an exploratory phase 2 trial, MBM patients received RT (stereotactic or whole-brain radiotherapy depending on the number of MBM) combined with ipilimumab (ipi) ± nivolumab (nivo) in different sequencing (Rad-ICI or ICI-Rad). Comparators arms included patients treated with ipi-free systemic treatment or without RT (in MBM-free patients). The primary endpoints were radiological and immunological responses in the peripheral blood. Secondary endpoints were progression-free survival (PFS) and overall survival (OS). Of 106 screened, 92 patients were included in the study. Multivariate analysis revealed an advantage for patients starting with RT (Rad-ICI) for overall response rate (RR: p = .007; HR: 7.88 (95%CI: 1.76-35.27)) and disease control rate (DCR: p = .036; HR: 6.26 (95%CI: 1.13-34.71)) with a trend for a better PFS (p = .162; HR: 1.64 (95%CI: 0.8-3.3)). After RT plus two cycles of ipi-based ICI in both RIT sequences, increased frequencies of activated CD4, CD8 T cells and an increase in melanoma-specific T cell responses were observed in the peripheral blood. Lasso regression analysis revealed a significant clinical benefit for patients treated with Rad-ICI sequence and immunological features, including high frequencies of memory T cells and activated CD8 T cells in the blood. This study supports increasing evidence that sequencing RT followed by ICI treatment may have better effects on the immunological responses and clinical outcomes in MBM patients.
Keywords: Melanoma; biomarkers; brain metastases; immune checkpoint inhibitors; immune monitoring; radiation; treatment sequence.
© 2022 The Author(s). Published with license by Taylor & Francis Group, LLC.
Conflict of interest statement
TES, HS, JM, DM, KL, MFH, IH, CK, RS, and PB declare no competing interests. JCH received scientific grant support from BMS; honoraria for talks from Almirall, Amgen, BMS, GSK, MSD, Novartis, Pfizer, Pierre Fabre, Roche, Sanofi; advisory board member for MSD, Pierre Fabre; travel grants from BMS, Immunocore, 4SC. MS received honoraria for talks from Novartis; travel grants from Merck, Abbvie, Novartis, Sanofi-Aventis, BMS, Merck Sharp & Dome, Pfizer. CM received a fellowship from the German Research Foundation (DFG) (ME 5482/1-1) 2/2020-5/2021. LK reports personal fees from Accuray Inc., and Novocure GmbH. AE received honoraria for Biotest AG, Meet the Experts, Janssen-Cilag, Klinikum Minden; consulting fees for Biotest AG, MSD, Galderma Laboratorium, Janssen-Cilag, Roche, AbbVie; advisory board member for MSD, Biotest. JD received grants from Viewray Inc, Accuray International Sari, RaySearch Laboratories AB, Vision RT Limited, Astellas Pharma GmbH, Siemens Healthcare GmbH, Solution Akademie GmbH, Egomed PLC Surrey Research Park, Quintiles GmbH, Pharmaceutical Research Associates GmbH, Boehringer Ingelheim Pharma GmbH&CoKG, PTW-Freiburg Dr. Pychlau GmbH, Nanobiotix S.A., Accuray Incorporated.
Figures



References
-
- Wolchok JD, Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob -J-J, Cowey CL, Lao CD, Wagstaff J, Schadendorf D, Ferrucci PF, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2017;377(14):1345–1356. published Online First: 2017/09/12. doi:10.1056/NEJMoa1709684. - DOI - PMC - PubMed
-
- Kluger HM, Chiang V, Mahajan A, Zito CR, Sznol M, Tran T, Weiss SA, Cohen JV, Yu J, Hegde U, et al. Long-Term survival of patients with melanoma with active brain metastases treated with pembrolizumab on a phase II Trial. J Clin Oncol. 2019;37(1):52–60. [published Online First: 2018/11/09]. doi:10.1200/jco.18.00204. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials