

Half-fluence Photodynamic Therapy for Central Serous Chorioretinopathy in a Patient Receiving Corticosteroids for Behçet's Uveitis
- PMID: 35481736
- PMCID: PMC9069094
- DOI: 10.4274/tjo.galenos.2022.96461
Half-fluence Photodynamic Therapy for Central Serous Chorioretinopathy in a Patient Receiving Corticosteroids for Behçet's Uveitis
Abstract
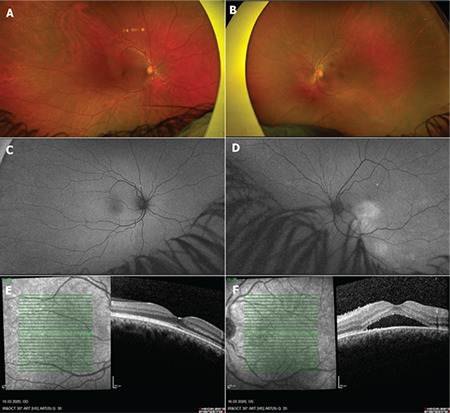
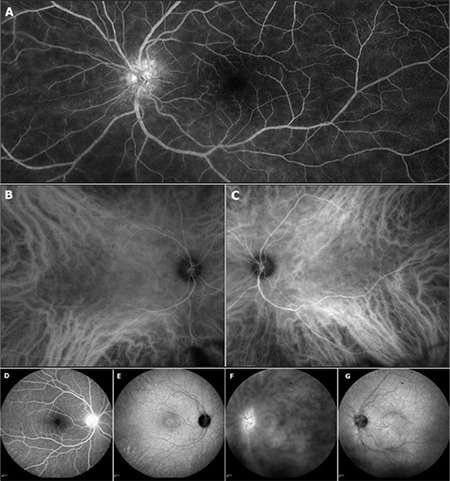
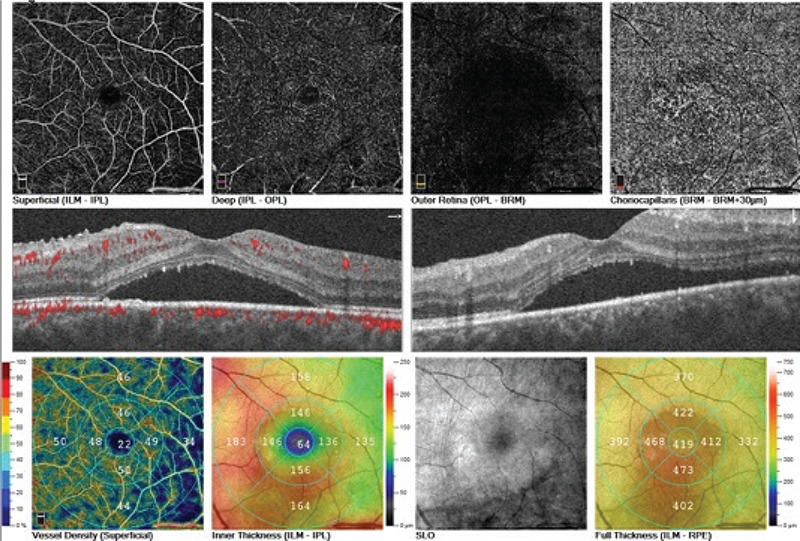
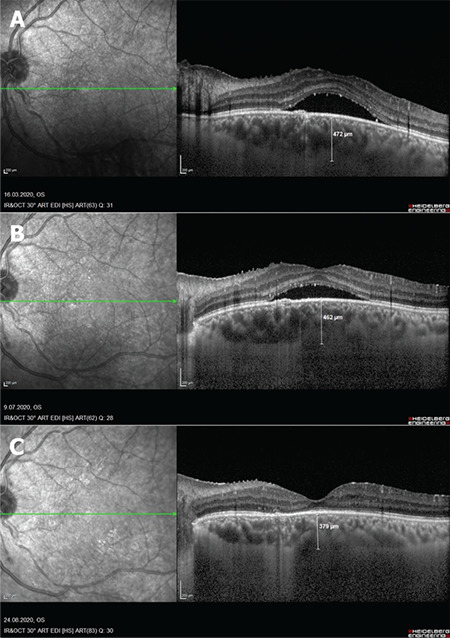
Corticosteroid-induced central serous chorioretinopathy (CSCR) has been reported to develop in many intraocular inflammatory diseases and usually resolves spontaneously after discontinuation of corticosteroids. Patients without any improvement may require alternative therapies. In this case report, we present the case of a 35-year-old man with Behçet's disease who had complaints of decreased vision due to CSCR in his left eye while using systemic corticosteroids along with cyclosporine and azathioprine. Half-fluence photodynamic therapy (PDT) was performed because the CSCR did not regress despite discontinuation of systemic corticosteroids. After treatment, his visual acuity increased with complete resolution of the subfoveal fluid. Half-fluence PDT seems to be an effective and safe treatment for patients who develop acute CSCR while under systemic or local corticosteroid therapy for intraocular inflammatory diseases such as Behçet's uveitis and do not improve despite steroid discontinuation.
Keywords: Behçet’s disease; central serous chorioretinopathy; photodynamic therapy; steroid; uveitis.
©Copyright 2022 by Turkish Ophthalmological Association, Turkish Journal of Ophthalmology, published by Galenos Publishing House.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures
References
-
- Khairallah M, Kahloun R, Tugal-Tutkun I. Central serous chorioretinopathy, corticosteroids, and uveitis. Ocul Immunol Inflamm. 2012;20:76–85. - PubMed
-
- Takayama K, Obata H, Takeuchi M. Efficacy of Adalimumab for Chronic Vogt-Koyanagi-Harada Disease Refractory to Conventional Corticosteroids and Immunosuppressive Therapy and Complicated by Central Serous Chorioretinopathy. Ocul Immunol Inflamm. 2020;28:509–512. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical