

Multiple congenital visceral abnormalities as a rare cause of pulmonary arterial hypertension
- PMID: 35482142
- PMCID: PMC9050997
- DOI: 10.1186/s43044-022-00273-x
Multiple congenital visceral abnormalities as a rare cause of pulmonary arterial hypertension
Abstract
Background: Pulmonary arterial hypertension (PAH) is a rare, progressive disorder. PAH is caused by a wide spectrum of pathologies but the cause remains undetermined on many occasions and patients are classified in the idiopathic group.
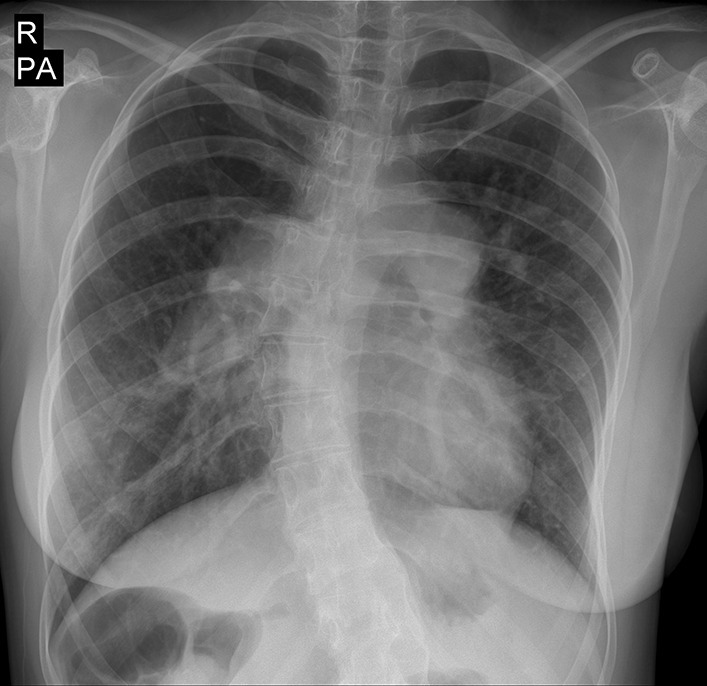
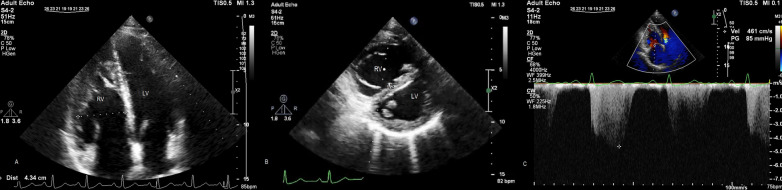
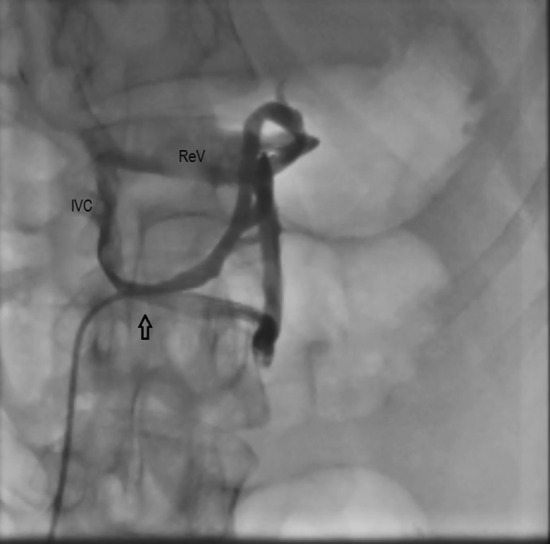
Case presentation: Here we report a young woman with rare congenital visceral abnormalities presenting with severe pulmonary hypertension.
Conclusions: Pulmonary hypertension is a complex disorder. Search for uncommon conditions that lead to pulmonary hypertension is necessary to determine the best management options.
Keywords: Abernethy malformation; Congenital heart disease; Mayer–Rokitansky–Küster–Hauser syndrome; Pulmonary hypertension.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37:67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
-
- Saedi S, Oraii S, Hajsheikholeslami F. A cross sectional study on prevalence and etiology of syncope in Tehran. Acta Med Iran. 2013;51(10):715–719. - PubMed
-
- Sakrana AA, Abdel Razek AAK, Yousef AM, El Tahlawi MA, Gadelhak BN. Cardiac magnetic resonance-derived indexed volumes and volume ratios of the cardiac chambers discriminating group 2 pulmonary hypertension from other World Health Organization groups. J Comput Assist Tomogr. 2021;45(1):59–64. doi: 10.1097/RCT.0000000000001058. - DOI - PubMed
LinkOut - more resources
Full Text Sources