

Where Are We Now and Where Might We Be Headed in Understanding and Managing Brain Metastases in Colorectal Cancer Patients?
- PMID: 35482170
- PMCID: PMC9174111
- DOI: 10.1007/s11864-022-00982-0
Where Are We Now and Where Might We Be Headed in Understanding and Managing Brain Metastases in Colorectal Cancer Patients?
Abstract
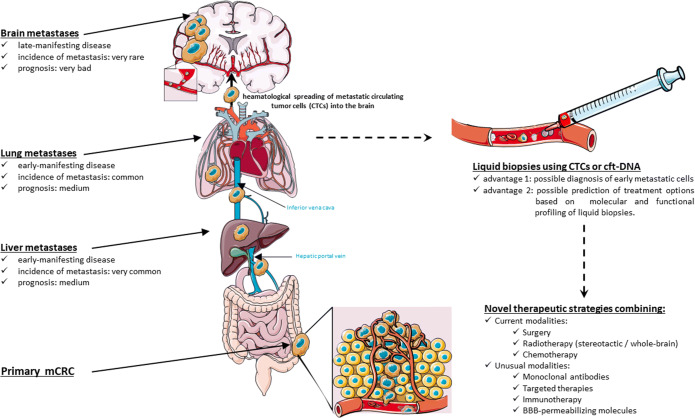
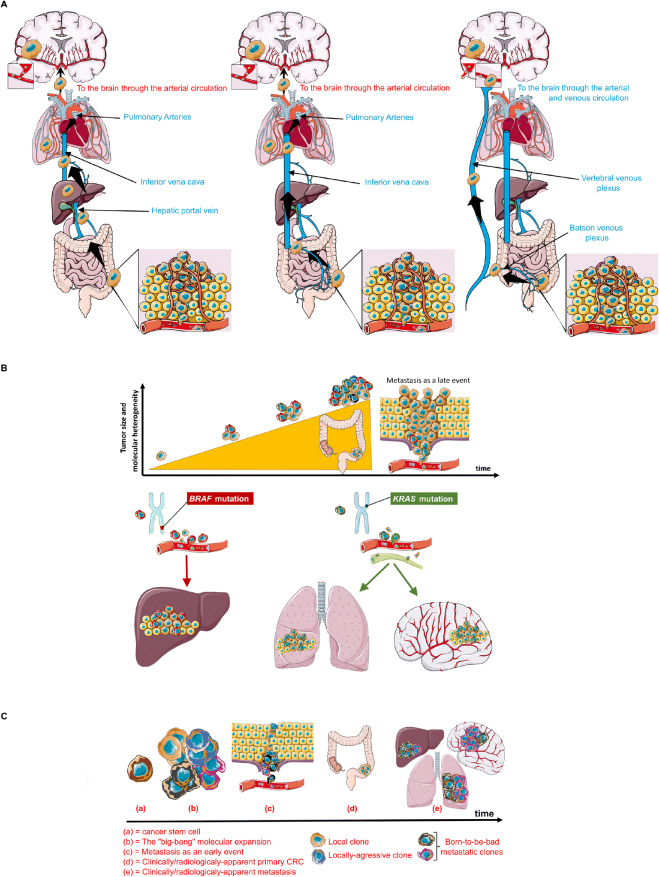
Opinion statement: Compared to liver and lung metastases, brain metastases (BMs) from colorectal cancer (CRC) are rare and remain poorly investigated despite the anticipated rise in their incidence. CRC patients bearing BM have a dismal prognosis with a median survival of 3-6 months, significantly lower than that of patients with BM from other primary tumors, and of those with metastatic CRC manifesting extracranially. While liver and lung metastases from CRC have more codified treatment strategies, there is no consensus regarding the treatment of BM in CRC, and their management follows the approaches of BM from other solid tumors. Therapeutic strategies are driven by the number and localisation of the lesion, consisting in local treatments such as surgery, stereotactic radiosurgery, or whole-brain radiotherapy. Novel treatment modalities are slowly finding their way into this shy unconsented armatorium including immunotherapy, monoclonal antibodies, tyrosine kinase inhibitors, or a combination of those, among others.This article reviews the pioneering strategies aiming at understanding, diagnosing, and managing this disease, and discusses future directions, challenges, and potential innovations in each of these domains.
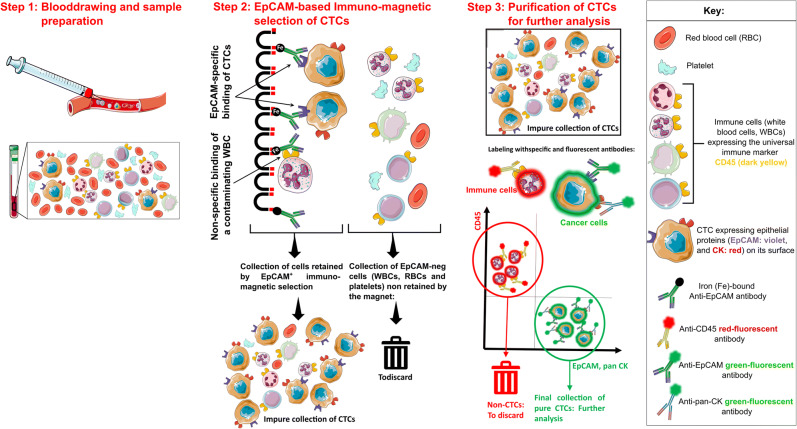
Highlights: • With the increasing survival in CRC, brain and other rare/late-onset metastases are rising. • Distal colon/rectal primary location, long-standing progressive lung metastases, and longer survival are risk factors for BM development in CRC. • Late diagnosis and lack of consensus treatment strategies make BM-CRC diagnosis very dismal. • Liquid biopsies using circulating tumor cells might offer excellent opportunities in the early diagnosis of BM-CRC and the search for therapeutic options. • Multi-modality treatment including surgical metastatic resection, postoperative SRS with/without WBRT, and chemotherapy is the best current treatment option. • Recent mid-sized clinical trials, case reports, and preclinical models show the potential of unconventional therapeutic approaches as monoclonal antibodies, targeted therapies, and immunotherapy. Graphical abstract.
Keywords: Brain metastasis (BM); Colorectal cancer (CRC); Liquid biopsies; Metastatic pathways; Novel treatments.
© 2022. The Author(s).
Conflict of interest statement
Thibaud Koessler discloses consulting and advisory role for Merck Sharp@Dohme (MSD), BMS, Lilly, Roche, Boehringer Ingelheim, and Servie. He has also benefited from Travel grants by Lilly, Ipsen, and Sanofi. The remaining authors have declared no conflicts of interest in connection with this article.
Figures
References
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
