

Advances in Clinical Cardiology 2021: A Summary of Key Clinical Trials
- PMID: 35482250
- PMCID: PMC9047629
- DOI: 10.1007/s12325-022-02136-y
Advances in Clinical Cardiology 2021: A Summary of Key Clinical Trials
Abstract
Introduction: Over the course of 2021, numerous key clinical trials with valuable contributions to clinical cardiology were published or presented at major international conferences. This review seeks to summarise these trials and reflect on their clinical context.
Methods: The authors reviewed clinical trials presented at major cardiology conferences during 2021 including the American College of Cardiology (ACC), European Association for Percutaneous Cardiovascular Interventions (EuroPCR), European Society of Cardiology (ESC), Transcatheter Cardiovascular Therapeutics (TCT), American Heart Association (AHA), European Heart Rhythm Association (EHRA), Society for Cardiovascular Angiography and Interventions (SCAI), TVT-The Heart Summit (TVT) and Cardiovascular Research Technologies (CRT). Trials with a broad relevance to the cardiology community and those with potential to change current practice were included.
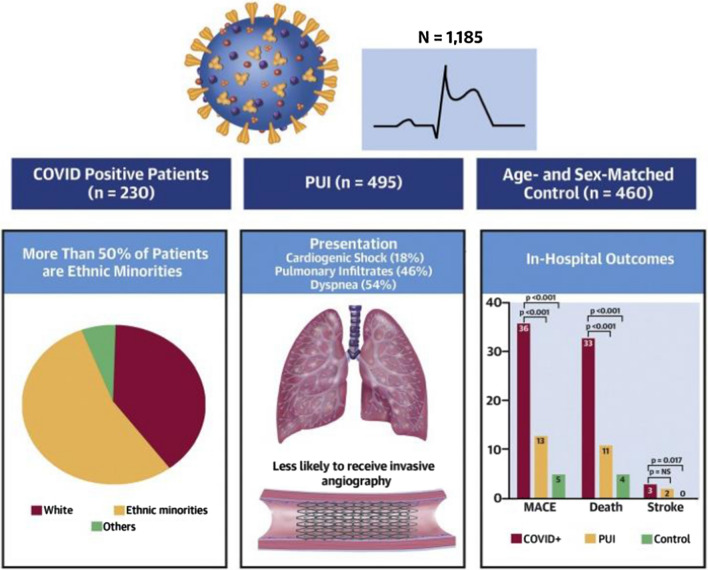
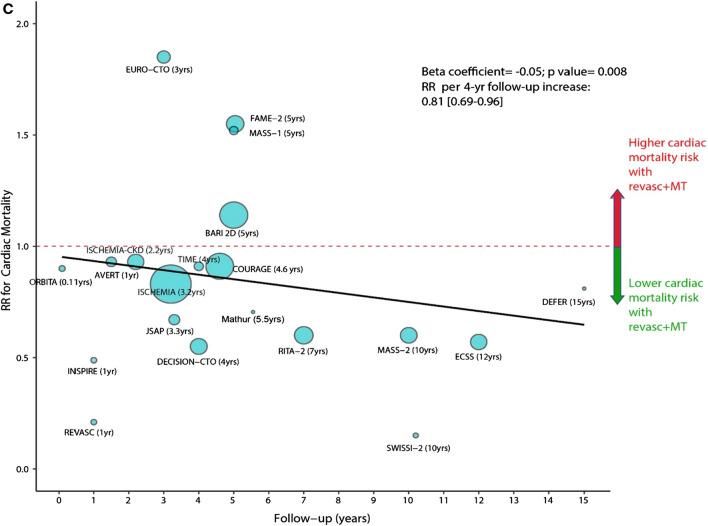
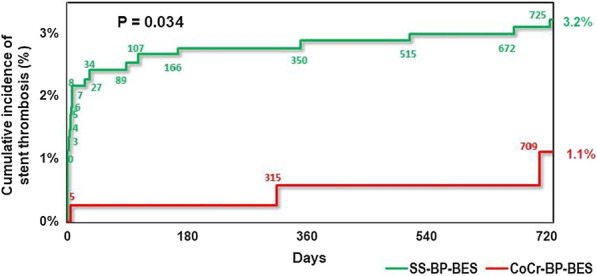
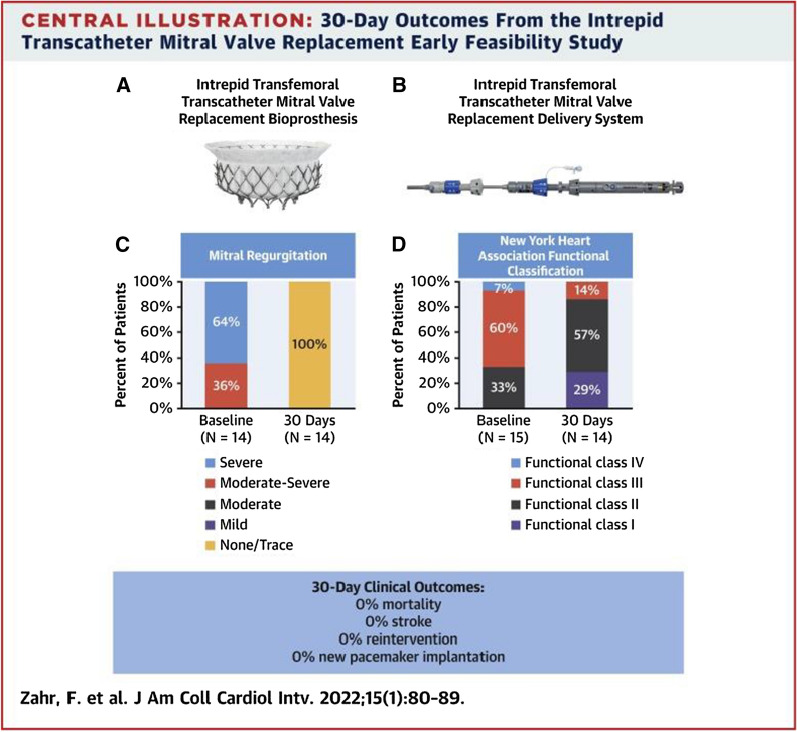
Results: A total of 150 key cardiology clinical trials were identified for inclusion. Interventional cardiology data included trials evaluating the use of new generation novel stent technology and new intravascular physiology strategies such as quantitative flow ratio (QFR) to guide revascularisation in stable and unstable coronary artery disease. New trials in acute coronary syndromes focused on shock, out of hospital cardiac arrest (OOHCA), the impact of COVID-19 on ST-elevation myocardial infarction (STEMI) networks and optimal duration/type of antiplatelet treatment. Structural intervention trials included latest data on transcatheter aortic valve replacement (TAVR) and mitral, tricuspid and pulmonary valve interventions. Heart failure data included trials with sodium-glucose cotransporter 2 (SGLT2) inhibitors, sacubitril/valsartan and novel drugs such as mavacamten for hypertrophic cardiomyopathy (HCM). Prevention trials included new data on proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors. In electrophysiology, new data regarding atrial fibrillation (AF) screening and new evidence for rhythm vs. rate control strategies were evaluated.
Conclusion: This article presents a summary of key clinical cardiology trials published and presented during the past year and should be of interest to both practising clinicians and researchers.
Keywords: Acute coronary syndrome; Antiplatelets; Atrial fibrillation; Cardiology; Coronary revascularisation; Heart failure; Left atrial appendage closure; Lipids; Mechanical support; Mitral clip; Shock; Transcatheter aortic valve implantation; Transcatheter tricuspid valve interventions.
© 2022. The Author(s).
Figures
References
-
- Abrahim C, Capitana A, Stanaway N, et al. Reducing EMS-to-balloon time—there's an app for that. J Am Coll Cardiol. 2021;77(18_suppl_2):16. doi: 10.1016/S0735-1097(21)01359-0. - DOI
-
- Mahmud E. Safety and efficacy of the second generation robotic-assisted system for percutaneous coronary intervention: final results of the multicenter PRECISION GRX study. Presented at SCAI 2021. April 29, 2021.
-
- Safirstein JG, Kowalski M, Chiu S, et al. Knowledge retention after percutaneous coronary intervention. J Am Coll Cardiol. 2021;77(18_suppl_1):968. doi: 10.1016/S0735-1097(21)02327-5. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
