

Gastric cancer complicated by paraneoplastic neurological syndrome which presented with extremity numbness: a case report
- PMID: 35482258
- PMCID: PMC9051002
- DOI: 10.1186/s40792-022-01429-2
Gastric cancer complicated by paraneoplastic neurological syndrome which presented with extremity numbness: a case report
Abstract
Background: Paraneoplastic neurological syndromes refer to a group of neurological disorders, which occur as distant effects of malignant tumors and are not caused by metastasis, nutritional disorders, or side effects of antitumor drugs.
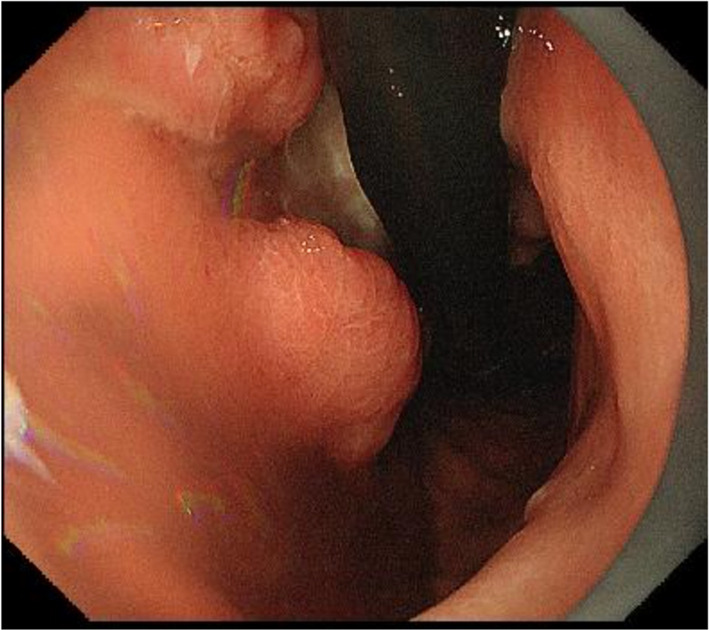
Case presentation: A 70-year-old woman complained of a 1-month history of extremity numbness. Upon presentation to our hospital, she had worsening numbness, and experienced staggering and falling. Physical examination revealed diminished tendon reflexes in both lower limbs, stocking and glove-type abnormal sensation, and left-sided dominant high-steppage gait due to weakness of the bilateral tibialis anterior muscles. Blood tests indicated anemia, and upper gastrointestinal endoscopy revealed gastric cancer, leading to laparoscopic distal gastrectomy. A nerve conduction velocity test showed demyelinating peripheral neuropathy. Further blood tests and imaging studies ruled out nutritional disorders, such as vitamin deficiency, diabetes-related diseases, connective tissue diseases, and central nervous system metastasis, leading to the suspicion of paraneoplastic neurological syndrome. After laparoscopic distal gastrectomy, the progression of symptoms stopped, and with intravenous high-dose immunoglobulin and steroid therapy, the symptoms improved to only minor numbness in the peripheral limbs as of the 18-month follow-up. As of the 2-year follow-up, there has been no cancer recurrence or metastasis.
Conclusions: When paraneoplastic neurological syndrome is suspected, early diagnosis and a multidisciplinary approach, including surgical treatment, are important before irreversible neurological damage occurs.
Keywords: Gastric cancer; Neurological disorder; Numbness; Paraneoplastic neurological syndrome.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Paraneoplastic neurological syndrome in a patient with gastric cancer.Gastric Cancer. 2010 Aug;13(3):204-8. doi: 10.1007/s10120-010-0563-2. Epub 2010 Sep 5. Gastric Cancer. 2010. PMID: 20820991
-
[A case of anti-Hu antibody- and anti-GluR epsilon2 antibody-positive paraneoplastic neurological syndrome presenting with limbic encephalitis and peripheral neuropathy].Rinsho Shinkeigaku. 2010 Jul;50(7):467-72. doi: 10.5692/clinicalneurol.50.467. Rinsho Shinkeigaku. 2010. PMID: 20681263 Japanese.
-
Anti-Ri-associated paraneoplastic ophthalmoplegia-ataxia syndrome in a woman with breast cancer: a case report and review of the literature.J Med Case Rep. 2020 Jun 12;14(1):67. doi: 10.1186/s13256-020-02410-z. J Med Case Rep. 2020. PMID: 32527295 Free PMC article. Review.
-
Neuroendocrine carcinoma of the small intestine diagnosed as a result of paraneoplastic neurological syndrome.Clin J Gastroenterol. 2023 Oct;16(5):663-667. doi: 10.1007/s12328-023-01822-w. Epub 2023 Jul 11. Clin J Gastroenterol. 2023. PMID: 37434043
-
Paraneoplastic Encephalopathy in a Patient With Metastatic Lung Cancer: A Case Study.J Adv Pract Oncol. 2018 Mar;9(2):216-221. Epub 2018 Mar 1. J Adv Pract Oncol. 2018. PMID: 30588355 Free PMC article. Review.
References
-
- Tanaka K. Paraneoplastic neurological syndromes with reference to anti-neuronal autoantibodies. Clin Neurol. 2010;50:371–378. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
