

Association of Open vs Robot-Assisted Radical Cystectomy With Mortality and Perioperative Outcomes Among Patients With Bladder Cancer in Sweden
- PMID: 35482309
- PMCID: PMC9051984
- DOI: 10.1001/jamanetworkopen.2022.8959
Association of Open vs Robot-Assisted Radical Cystectomy With Mortality and Perioperative Outcomes Among Patients With Bladder Cancer in Sweden
Abstract
Importance: Mortality rates resulting from bladder cancer have remained unchanged for more than 30 years. The surgical community has put hope in robot-assisted radical cystectomy (RARC) with intracorporeal urinary diversion (ICUD) in an effort to improve surgical outcomes and bladder cancer survival without strong supporting evidence.
Objective: To evaluate perioperative, safety, and survival outcome differences between RARC with ICUD and open radical cystectomy (ORC).
Design, setting, and participants: This nationwide population-based cohort study used data from the Swedish National Register of Urinary Bladder Cancer and population-based Cause of Death Register, which includes clinical information on tumor characteristics, treatment, and survival and covers approximately 97% of patients with urinary bladder cancer in Sweden. All patients who underwent radical cystectomy for bladder cancer in any hospital between January 2011 and December 2018 were included. Follow-up data were collected until December 2019. Data analysis was conducted from June to December 2020.
Exposures: RARC or ORC.
Main outcomes and measures: The main outcomes were all-cause and cancer-specific mortality between RARC and ORC, compared using propensity score matching. Secondary outcomes were differences in perioperative outcomes after the different surgical approaches.
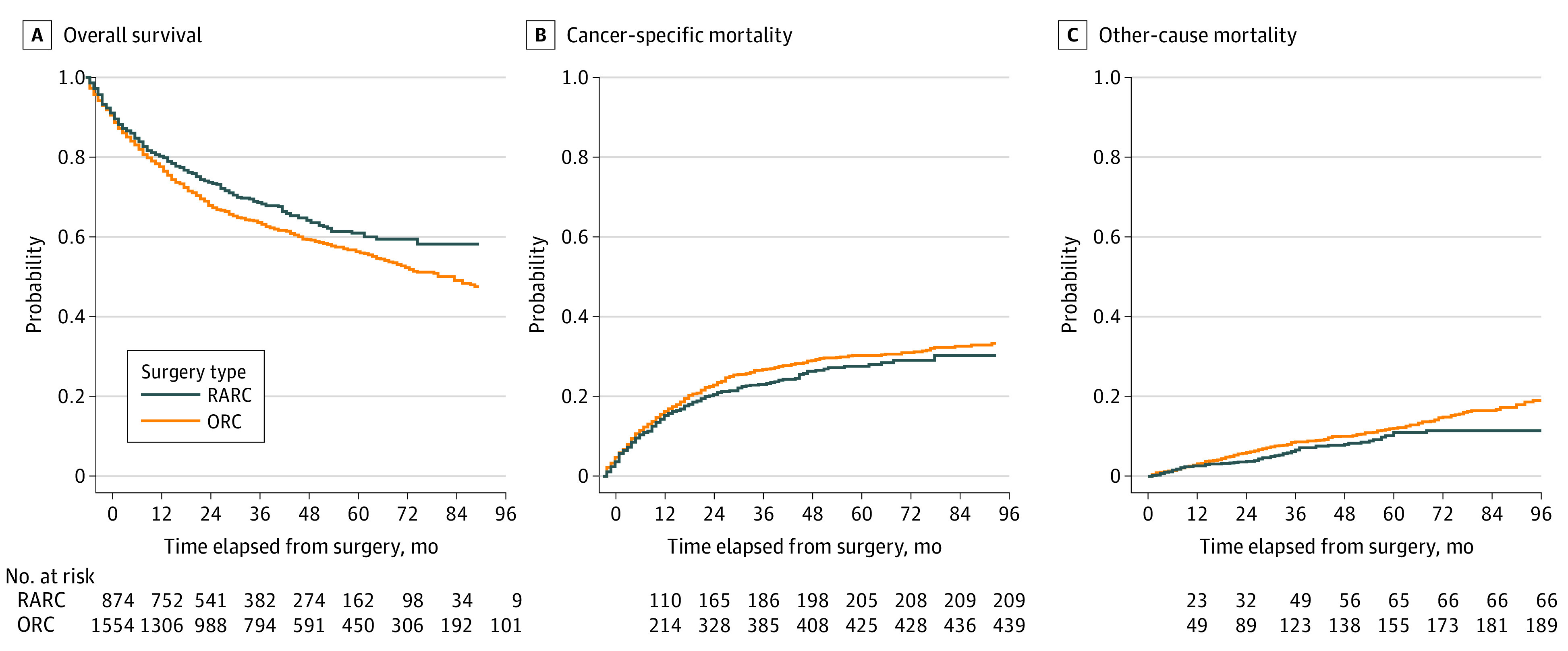
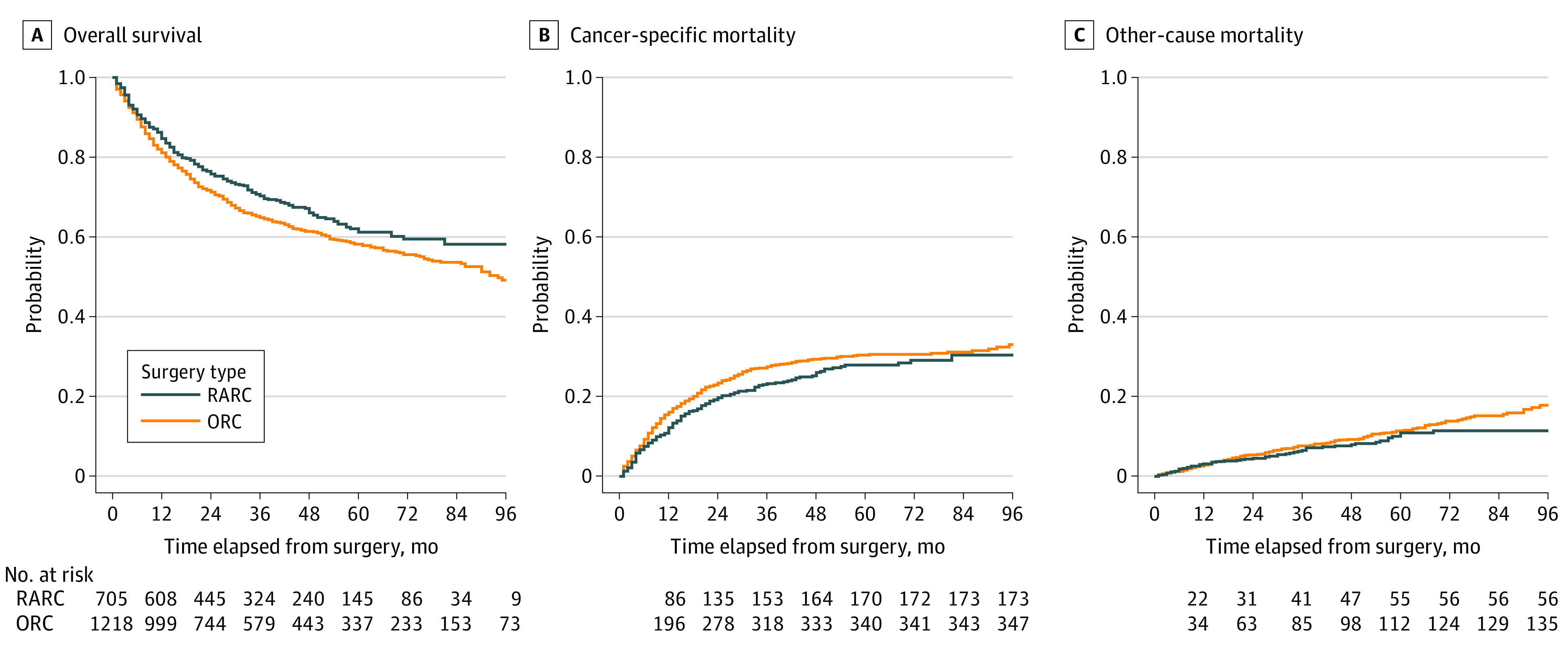
Results: Throughout the observation period, 889 patients underwent RARC and 2280 patients underwent ORC at 24 Swedish hospitals. The median (IQR) age was 71 (66-76) years and 2386 patients (75.3%) were men. After a median (IQR) follow-up of 47 (28-71) months, the 5-year cancer-specific mortality rates were 30.2% (variance, 1.59) for ORC and 27.6% (variance, 3.12) for RARC, and the overall survival rates were 57.7% (variance, 2.46) for ORC and 61.4% (variance, 5.11) for RARC. In the propensity score-matched analysis, RARC was associated with a lower all-cause mortality (hazard ratio, 0.71; 95% CI, 0.56-0.89; P = .004). Compared with ORC, RARC was associated with a lower estimated blood loss (median [IQR] 150 [100-300] mL vs 700 [400-1300] mL; P < .001), intraoperative transfusion rate (odds ratio [OR], 0.05; 95% CI, 0.03-0.08; P < .001), and shorter length of stay (median [IQR], 9 [6-13] days vs 13 [10-17] days; P < .001), and with a higher lymph node yield (median [IQR], 20 [15-27] lymph nodes vs 14 [8-24] lymph nodes; P < .001) and 90-day rehospitalization rate (OR, 1.28; 95% CI, 1.02-1.60; P = .03). The RARC group, compared with the ORC group had lower risk of Clavien-Dindo grade III or higher complications (OR, 0.62; 95% CI, 0.43-0.87; P = .009).
Conclusions and relevance: These findings suggest that compared with ORC, RARC with ICUD was associated with a lower overall mortality rate, fewer high-grade complications, and more favorable perioperative outcomes.
Conflict of interest statement
Figures
References
-
- Zamboni S, Soria F, Mathieu R, et al. ; European Association of Urology - Young Academic Urologists (EAU-YAU), Urothelial carcinoma working group . Differences in trends in the use of robot-assisted and open radical cystectomy and changes over time in peri-operative outcomes among selected centres in North America and Europe: an international multicentre collaboration. BJU Int. 2019;124(4):656-664. doi: 10.1111/bju.14791 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
