

Hypertensive Disorders in Pregnancy and Mortality at Delivery Hospitalization - United States, 2017-2019
- PMID: 35482575
- PMCID: PMC9098235
- DOI: 10.15585/mmwr.mm7117a1
Hypertensive Disorders in Pregnancy and Mortality at Delivery Hospitalization - United States, 2017-2019
Abstract
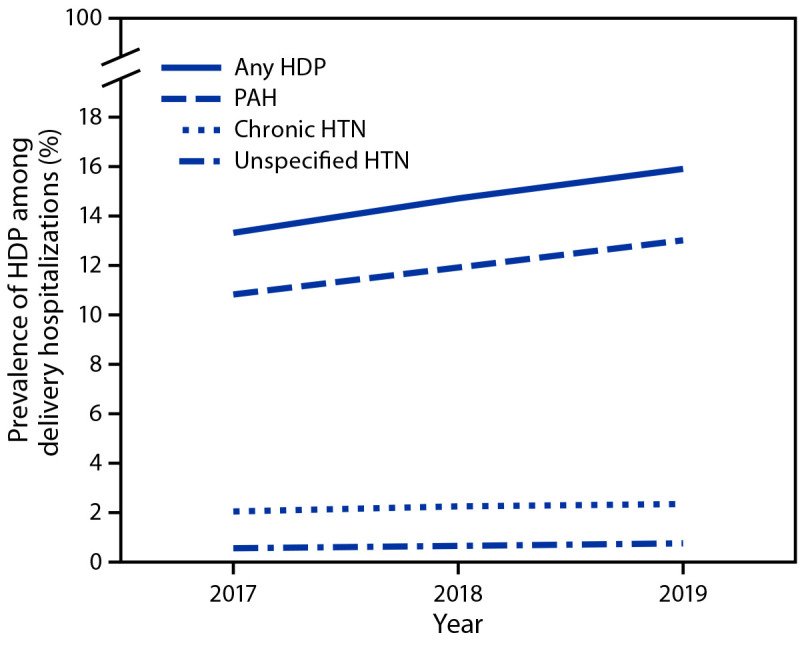
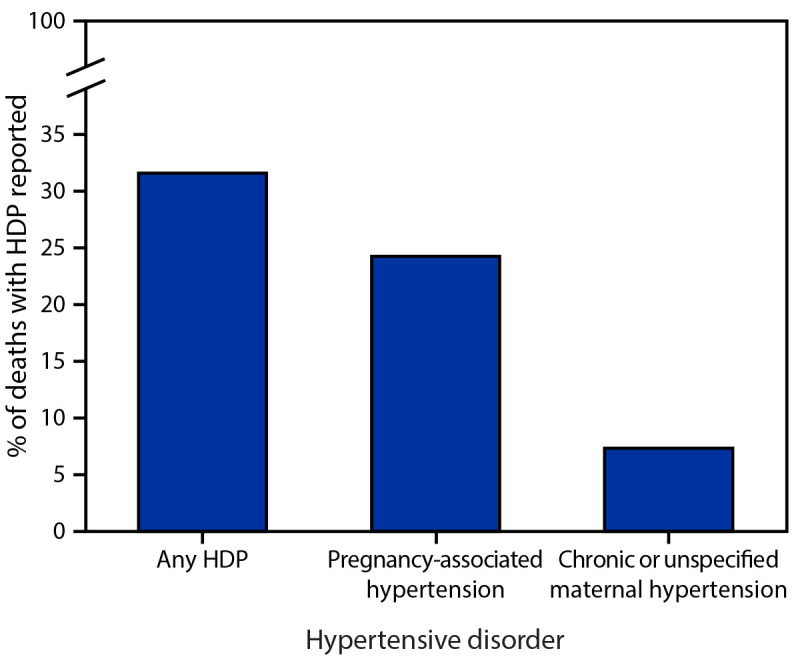
Hypertensive disorders in pregnancy (HDPs), defined as prepregnancy (chronic) or pregnancy-associated hypertension, are common pregnancy complications in the United States.* HDPs are strongly associated with severe maternal complications, such as heart attack and stroke (1), and are a leading cause of pregnancy-related death in the United States.† CDC analyzed nationally representative data from the National Inpatient Sample to calculate the annual prevalence of HDP among delivery hospitalizations and by maternal characteristics, and the percentage of in-hospital deaths with an HDP diagnosis code documented. During 2017-2019, the prevalence of HDP among delivery hospitalizations increased from 13.3% to 15.9%. The prevalence of pregnancy-associated hypertension increased from 10.8% in 2017 to 13.0% in 2019, while the prevalence of chronic hypertension increased from 2.0% to 2.3%. Prevalence of HDP was highest among delivery hospitalizations of non-Hispanic Black or African American (Black) women, non-Hispanic American Indian and Alaska Native (AI/AN) women, and women aged ≥35 years, residing in zip codes in the lowest median household income quartile, or delivering in hospitals in the South or the Midwest Census regions. Among deaths that occurred during delivery hospitalization, 31.6% had any HDP documented. Clinical guidance for reducing complications from HDP focuses on prompt identification and preventing progression to severe maternal complications through timely treatment (1). Recommendations for identifying and monitoring pregnant persons with hypertension include measuring blood pressure throughout pregnancy,§ including self-monitoring. Severe complications and mortality from HDP are preventable with equitable implementation of strategies to identify and monitor persons with HDP (1) and quality improvement initiatives to improve prompt treatment and increase awareness of urgent maternal warning signs (2).
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- Garovic VD, Dechend R, Easterling T, et al.; American Heart Association Council on Hypertension; Council on the Kidney in Cardiovascular Disease, Kidney in Heart Disease Science Committee; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Lifestyle and Cardiometabolic Health; Council on Peripheral Vascular Disease; Stroke Council. Hypertension in pregnancy: diagnosis, blood pressure goals, and pharmacotherapy: a scientific statement from the American Heart Association. Hypertension 2022;79:e21–41. 10.1161/HYP.0000000000000208 - DOI - PMC - PubMed
