

Harnessing Big Data to Advance Treatment and Understanding of Pulmonary Hypertension
- PMID: 35482840
- PMCID: PMC9070103
- DOI: 10.1161/CIRCRESAHA.121.319969
Harnessing Big Data to Advance Treatment and Understanding of Pulmonary Hypertension
Abstract
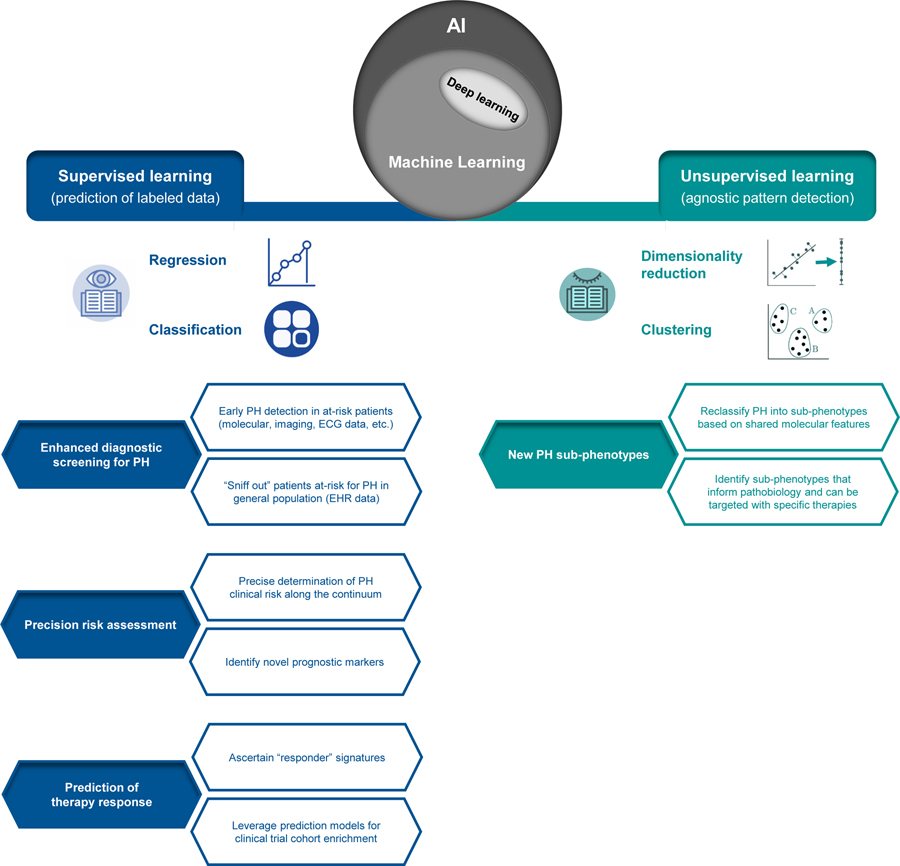
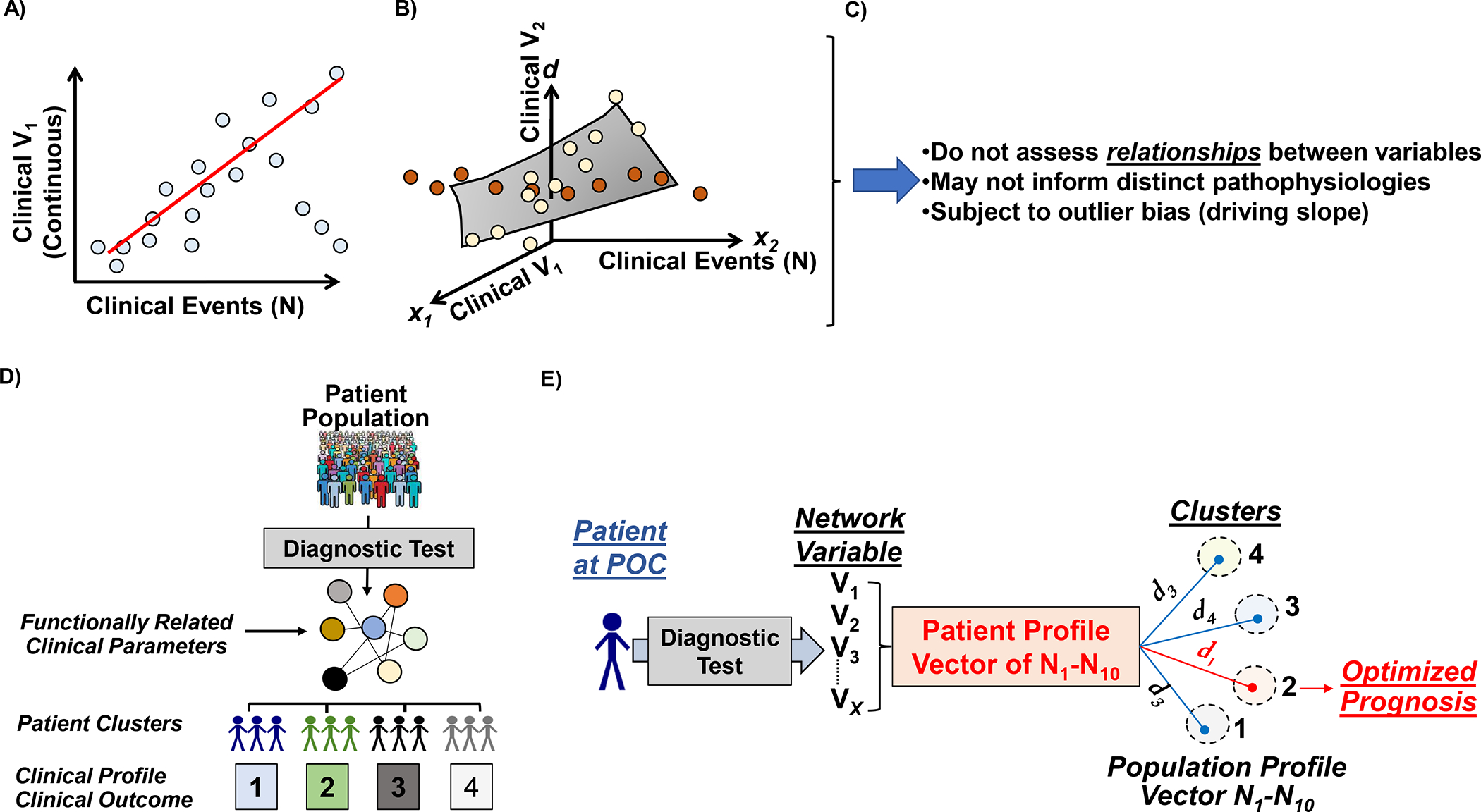
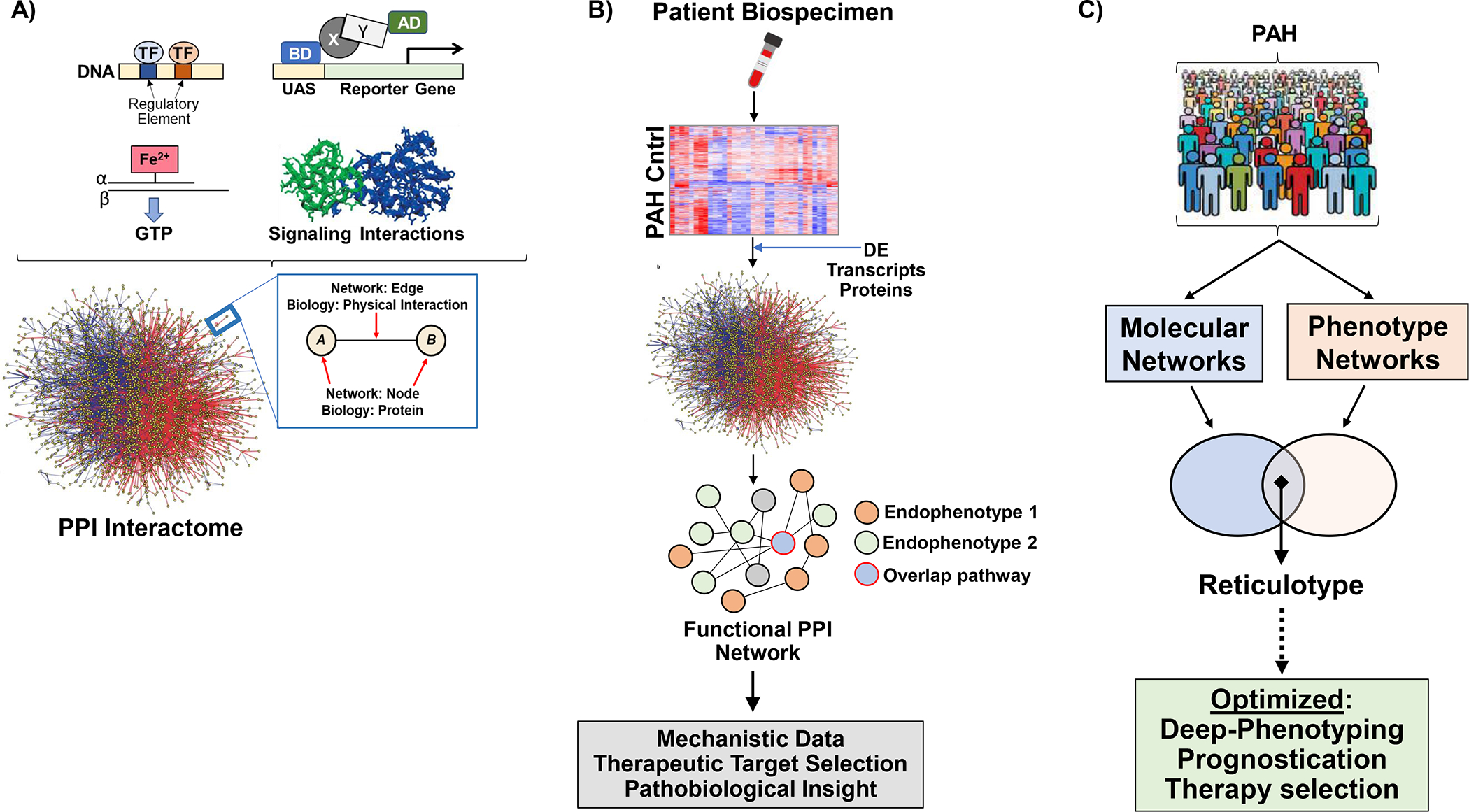
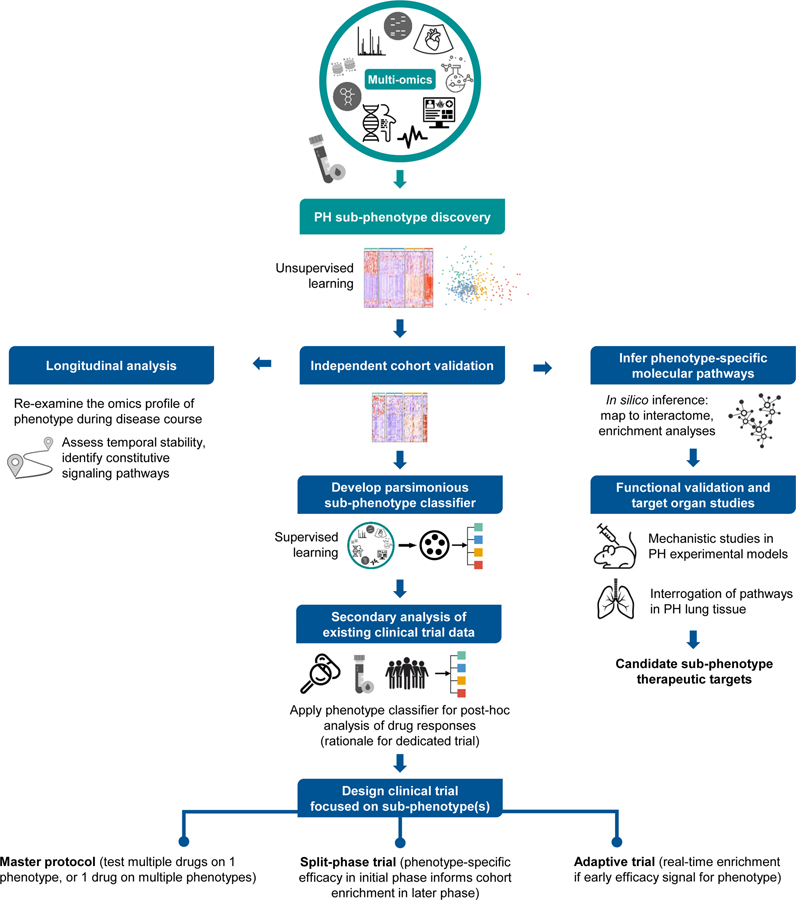
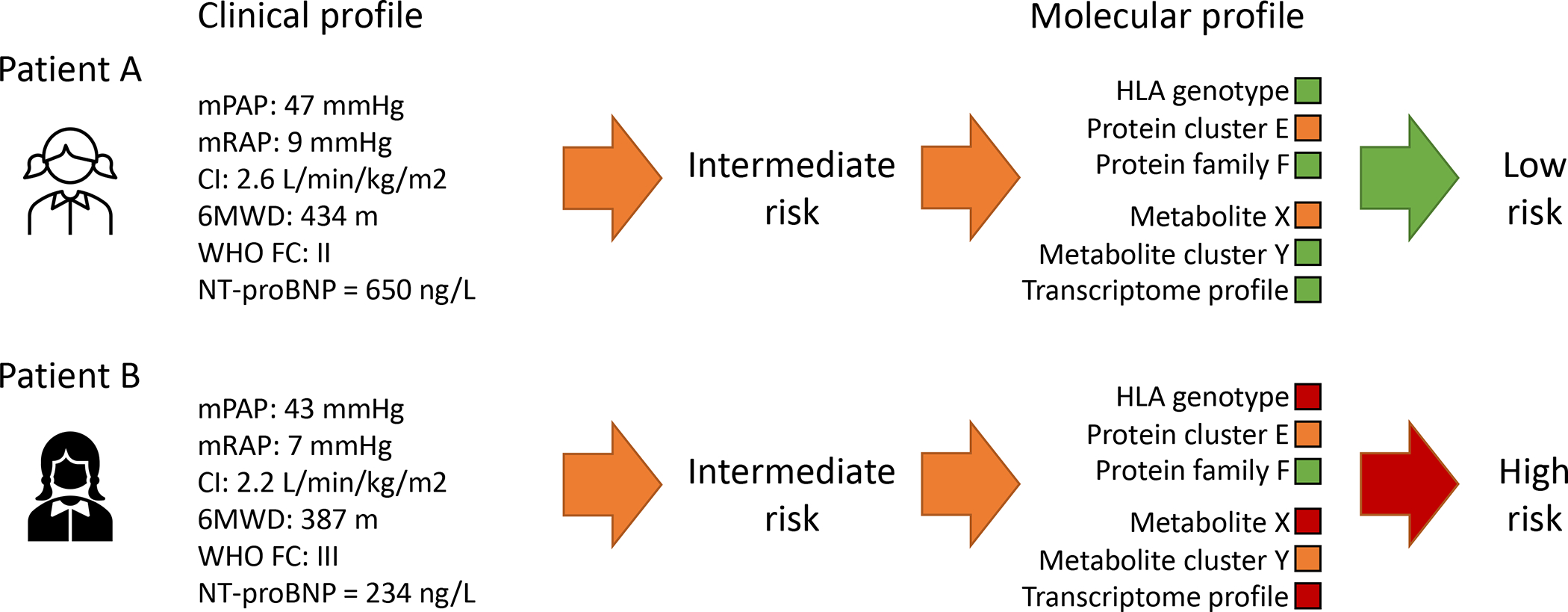
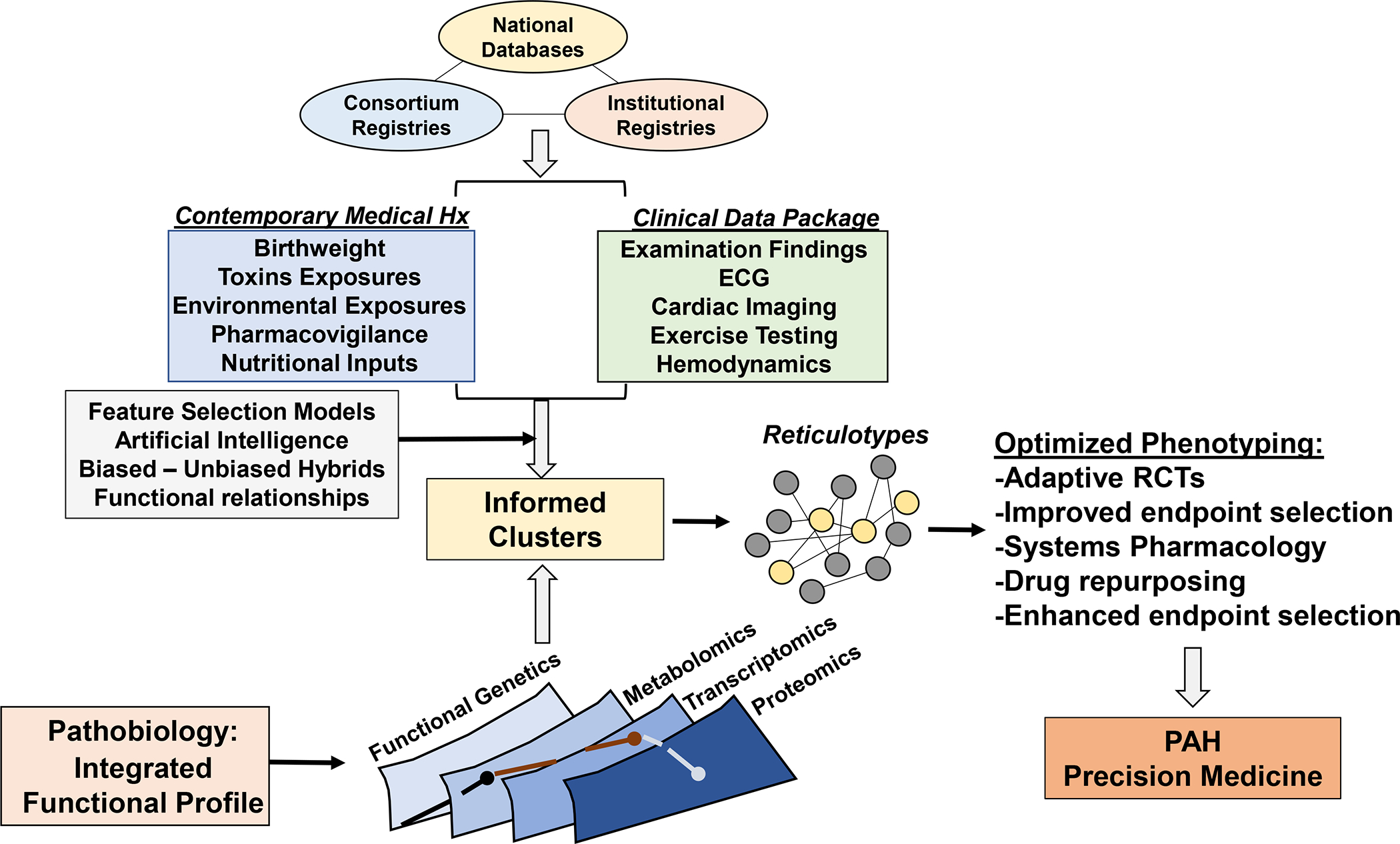
Pulmonary hypertension is a complex disease with multiple causes, corresponding to phenotypic heterogeneity and variable therapeutic responses. Advancing understanding of pulmonary hypertension pathogenesis is likely to hinge on integrated methods that leverage data from health records, imaging, novel molecular -omics profiling, and other modalities. In this review, we summarize key data sets generated thus far in the field and describe analytical methods that hold promise for deciphering the molecular mechanisms that underpin pulmonary vascular remodeling, including machine learning, network medicine, and functional genetics. We also detail how genetic and subphenotyping approaches enable earlier diagnosis, refined prognostication, and optimized treatment prediction. We propose strategies that identify functionally important molecular pathways, bolstered by findings across multi-omics platforms, which are well-positioned to individualize drug therapy selection and advance precision medicine in this highly morbid disease.
Keywords: big data; information dissemination; phenotype; precision medicine; pulmonary arterial hypertension.
Conflict of interest statement
Figures
References
-
- Southgate L, Machado RD, Graf S and Morrell NW. Molecular genetic framework underlying pulmonary arterial hypertension. Nature reviews Cardiology. 2019. - PubMed
-
- Zhu N, Swietlik EM, Welch CL, Pauciulo MW, Hagen JJ, Zhou X, Guo Y, Karten J, Pandya D, Tilly T, et al. Rare variant analysis of 4241 pulmonary arterial hypertension cases from an international consortium implicates FBLN2, PDGFD, and rare de novo variants in PAH. Genome Med. 2021;13:80. - PMC - PubMed
-
- Wu Y, Wharton J, Walters R, Vasilaki E, Aman J, Zhao L, Wilkins MR and Rhodes CJ. The pathophysiological role of novel pulmonary arterial hypertension gene SOX17. Eur Respir J. 2021;58. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
