

Effects of non-invasive respiratory supports on inspiratory effort in moderate-severe COVID-19 patients. A randomized physiological study
- PMID: 35483993
- PMCID: PMC9023341
- DOI: 10.1016/j.ejim.2022.04.012
Effects of non-invasive respiratory supports on inspiratory effort in moderate-severe COVID-19 patients. A randomized physiological study
Abstract
Rationale and objective: Various forms of Non-invasive respiratory support (NRS) have been used during COVID-19, to treat Hypoxemic Acute Respiratory Failure (HARF), but it has been suggested that the occurrence of strenuous inspiratory efforts may cause Self Induced Lung Injury(P-SILI). The aim of this investigation was to record esophageal pressure, when starting NRS application, so as to better understand the potential risk of the patients in terms of P-SILI and ventilator induced lung injury (VILI).
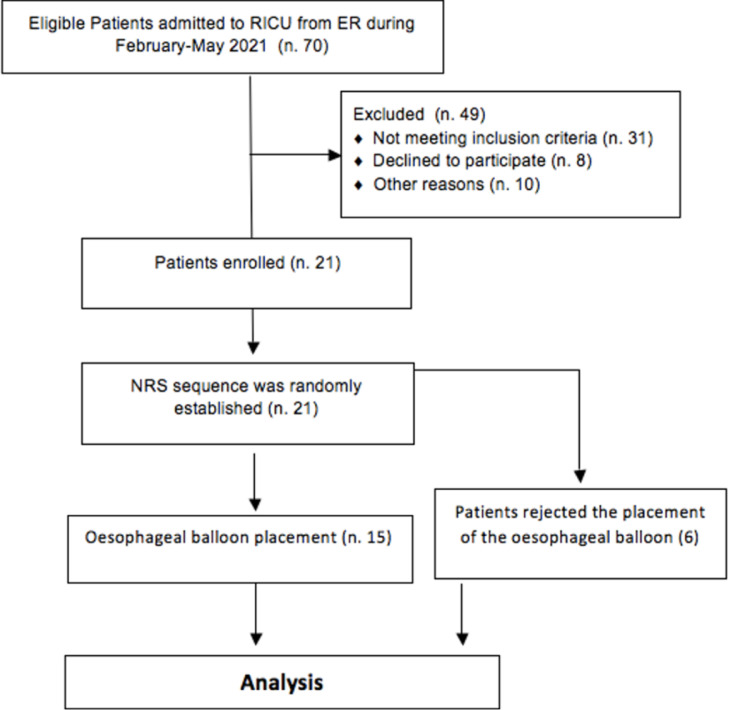
Methods and measurements: 21 patients with early de-novo respiratory failure due to COVID-19, underwent three 30 min trials applied in random order: high-flow nasal cannula (HFNC), continuous positive airway pressure (CPAP), and non-invasive ventilation (NIV). After each trial, standard oxygen therapy was reinstituted using a Venturi mask (VM). 15 patients accepted a nasogastric tube placement. Esophageal Pressure (ΔPes) and dynamic transpulmonary driving pressure (ΔPLDyn), together with the breathing pattern using a bioelectrical impedance monitor were recorded. Arterial blood gases were collected in all patients.
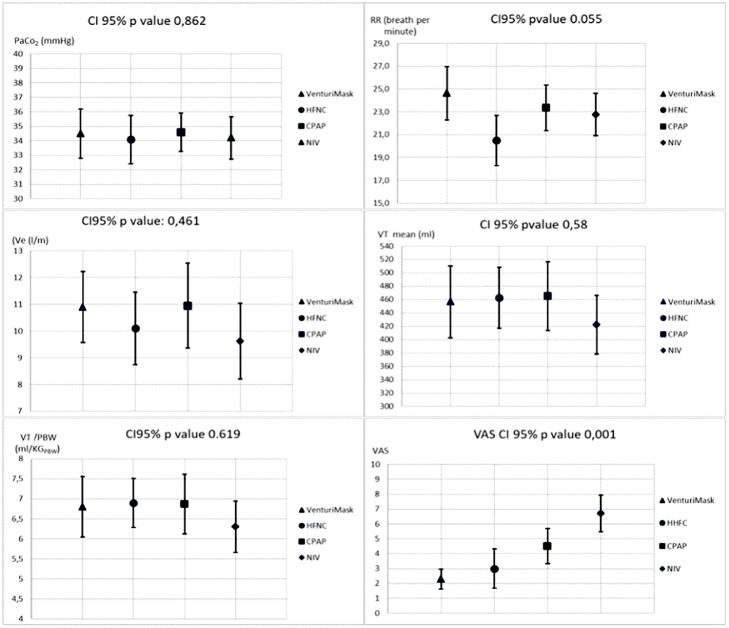
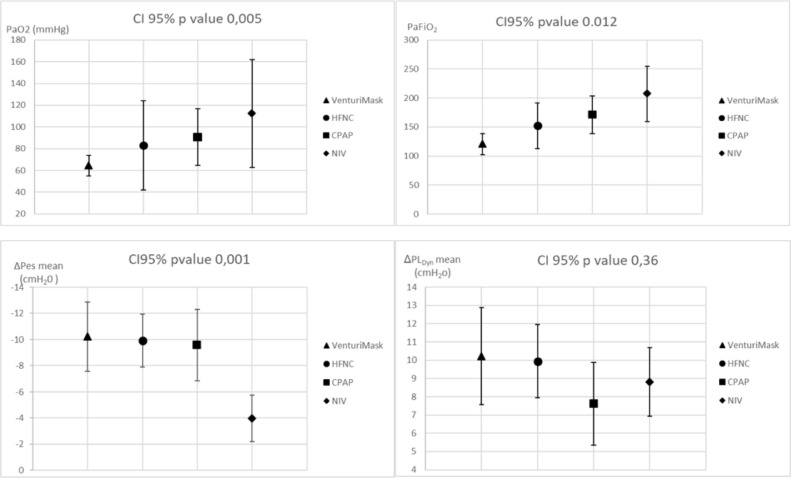
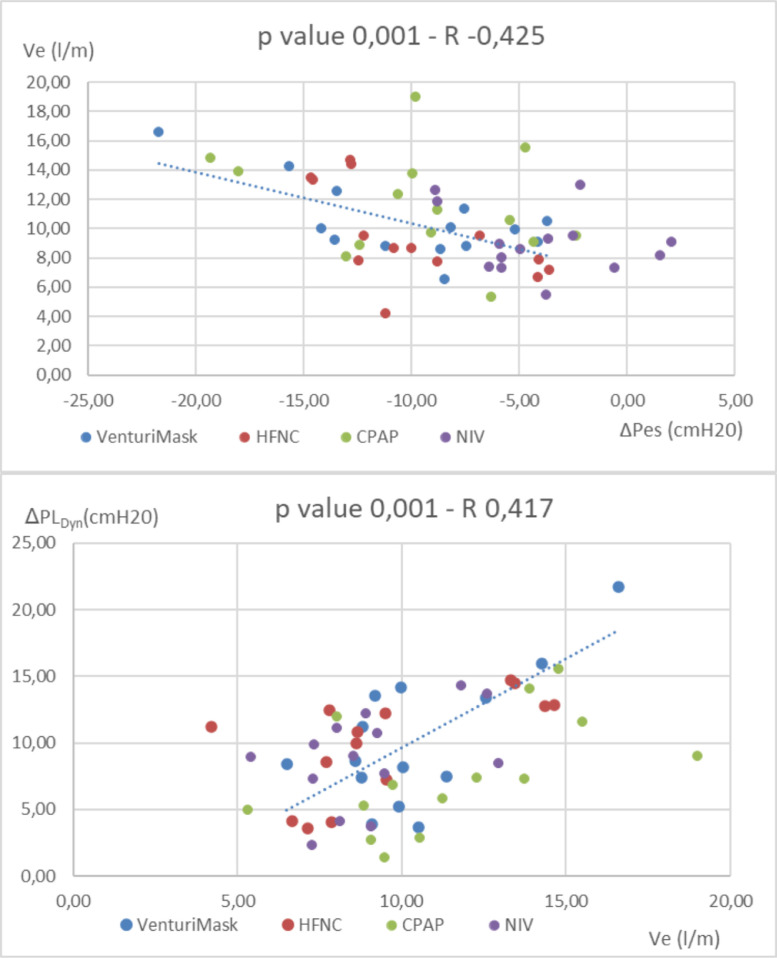
Main results: No statistically significant differences in breathing pattern and PaCO2 were found. PaO2/FiO2 ratio improved significantly during NIV and CPAP vs VM. NIV was the only NRS to reduce significantly ΔPes vs. VM (-10,2 ±5 cmH20 vs -3,9 ±3,4). No differences were found in ΔPLDyn between NRS (10,2±5; 9,9±3,8; 7,6±4,3; 8,8±3,6 during VM, HFNC, CPAP and NIV respectively). Minute ventilation (Ve) was directly dependent on the patient's inspiratory effort, irrespective of the NRS applied. 14% of patients were intubated, none of them showing a reduction in ΔPes during NRS.
Conclusions: In the early phase of HARF due to COVID-19, the inspiratory effort may not be markedly elevated and the application of NIV and CPAP ameliorates oxygenation vs VM. NIV was superior in reducing ΔPes, maintaining ΔPLDyn within a range of potential safety.
Keywords: COVID 19; Hypoxemic acute respiratory failure; Non invasive respiratory supports.
Copyright © 2022. Published by Elsevier B.V.
Figures
Comment in
-
Non-invasive respiratory supports on inspiratory effort in Covid-19: how and when is it matter of selection?Eur J Intern Med. 2022 Oct;104:107-108. doi: 10.1016/j.ejim.2022.08.026. Epub 2022 Aug 22. Eur J Intern Med. 2022. PMID: 36055956 Free PMC article. No abstract available.
-
Non-invasive respiratory supports on inspiratory effort in COVID-19: How and when is it matter of selection? Author's reply.Eur J Intern Med. 2022 Oct;104:109. doi: 10.1016/j.ejim.2022.08.034. Epub 2022 Sep 1. Eur J Intern Med. 2022. PMID: 36057528 Free PMC article. No abstract available.
References
-
- Brambilla AM, Aliberti S, Prina E, et al. Helmet CPAP vs. oxygen therapy in severe hypoxemic respiratory failure due to pneumonia. Intensive Care Med. 2014;40(7):942–949. Erratum in: Intensive Care Med. 2014 Aug;40(8):1187. PMID: 24817030. - PubMed
-
- Frat J-P, Thille AW, Mercat A, et al; FLORALI Study Group; REVA Network. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015 ;372(23):2185-96. - PubMed
-
- Jaber S, Lescot T, Futier E, et al. NIVAS Study Group. Effect of noninvasive ventilation on tracheal reintubation among patients with hypoxemic respiratory failure following abdominal surgery: a randomized clinical trial. JAMA. 2016;315(13): 1345-1353. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
