

Molecular pathogenesis and systemic therapies for hepatocellular carcinoma
- PMID: 35484418
- PMCID: PMC9060366
- DOI: 10.1038/s43018-022-00357-2
Molecular pathogenesis and systemic therapies for hepatocellular carcinoma
Abstract
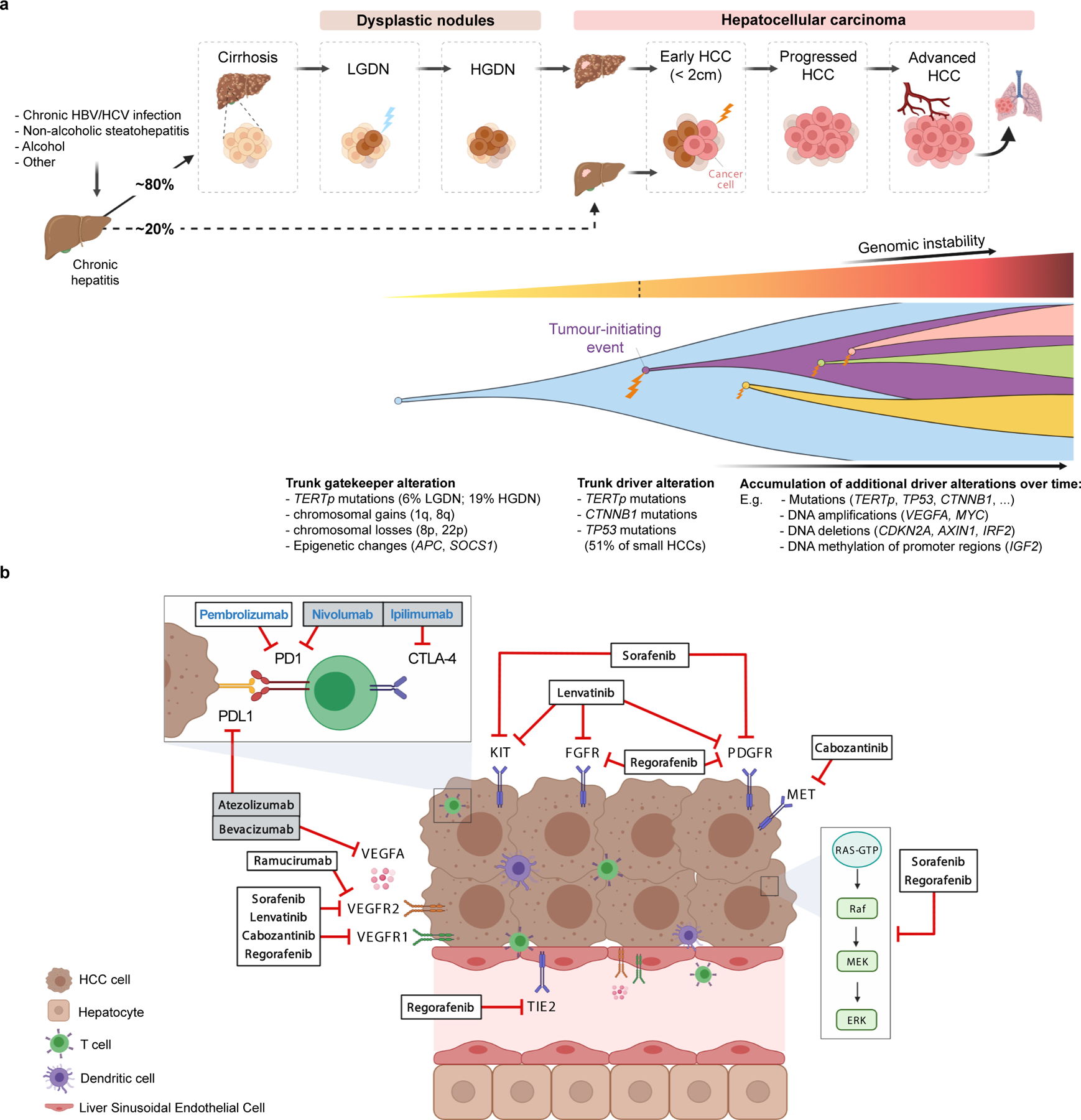
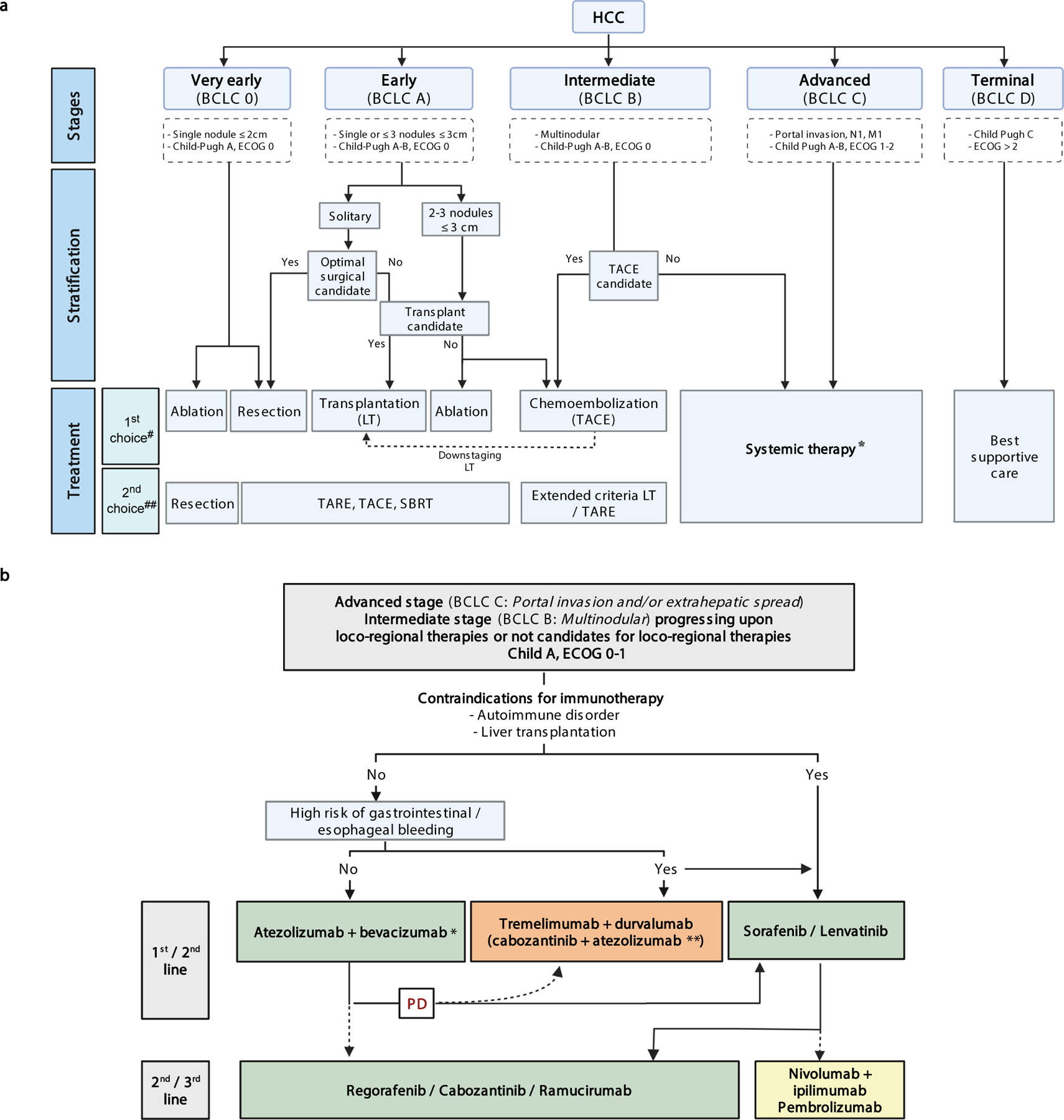
Hepatocellular carcinoma (HCC) remains one of the most prevalent and deadliest cancers. The poor outcome associated with HCC is dramatically changing due to the advent of effective systemic therapies. Here we discuss the molecular pathogenesis of HCC, molecular classes and determinants of heterogeneity. In addition, effective single-agent and combination systemic therapies involving immunotherapies as standard of care are analyzed. Finally, we propose a flowchart of sequential therapies, explore mechanisms of resistance and address the need for predictive biomarkers.
© 2022. Springer Nature America, Inc.
Conflict of interest statement
Competing interests
J.M.L received research support from Bayer HealthCare Pharmaceuticals, Eisai Inc, Boehringer-Ingelheim and Ipsen, and consulting fees from Merck, Eli Lilly, Eisai Inc, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb, Ipsen, Genentech, Roche, Glycotest, Nucleix, Omega Therapeutics, Iylon, Mina Alpha Ltd, Boston Scientific and AstraZeneca. H.R. has acted in an advisory capacity for Boston Scientific and Sirtex, as well as receiving speaker fees from Eisai and Bayer. A.V. has received consulting fees from Boehringer Ingelheim, FirstWorld, Natera, Cambridge Healthcare Research and Genentech; advisory board fees from Bristol Myers-Squibb, Gilead and NGM Pharmaceuticals; and research support from Eisai. R.K.K. received research support from Agios, Astra Zeneca, Bayer, Bristol Myers-Squibb, Eli Lilly, EMD Serono, Exelixis, Genentech/Roche, Merck, Partner Therapeutics, Novartis, QED, Relay Therapeutics, Surface Oncology and Taiho; and consulting/advisory fees from Exact Sciences, Genentech/Roche and Gilead. A.E-K. has received research support from Astex, Astrazeneca, and Fulgent; advisory or consulting fees from Bayer, Bristol Myers-Squibb, EISAI, Merck, Exelixis, Astrazeneca, Roche/Genentech, Agenus, ABL Bio, QED, Gilead, Cytomx, Pieris, and EMD Serono. G.G., X.W.W. and R.P. have no competing interests.
Figures
References
-
- Llovet JM et al. Hepatocellular carcinoma. Nat. Rev. Dis. Prim 7, 7 (2021). - PubMed
-
- Villanueva A Hepatocellular Carcinoma. N. Engl. J. Med 380, 1450–1462 (2019). - PubMed
-
- Zucman-Rossi J, Villanueva A, Nault JC & Llovet JM Genetic Landscape and Biomarkers of Hepatocellular Carcinoma. Gastroenterology 149, 1226–1239 (2015). - PubMed
