

Effect of In-Person Delivered Behavioural Interventions in People with Multimorbidity: Systematic Review and Meta-analysis
- PMID: 35484462
- PMCID: PMC10036283
- DOI: 10.1007/s12529-022-10092-8
Effect of In-Person Delivered Behavioural Interventions in People with Multimorbidity: Systematic Review and Meta-analysis
Abstract
Background: To investigate the effect of in-person delivered behavioural interventions in people with multimorbidity and which behaviour change techniques (BCTs), targeting lifestyle behaviours, are associated with better outcomes.
Methods: Systematic review of randomised controlled trials. We searched MEDLINE, EMBASE, CENTRAL, and CINAHL and screened reference list of reviews including people with multimorbidity, registries, and citation tracking of included studies. Meta-analyses using random-effects model to assess the effect of behavioural interventions and meta-regression analyses and effectiveness ratios to investigate the impact of mediators on effect estimates. Cochrane 'Risk of Bias Tool' 2.0 and the GRADE assessment to evaluate the overall quality of evidence.
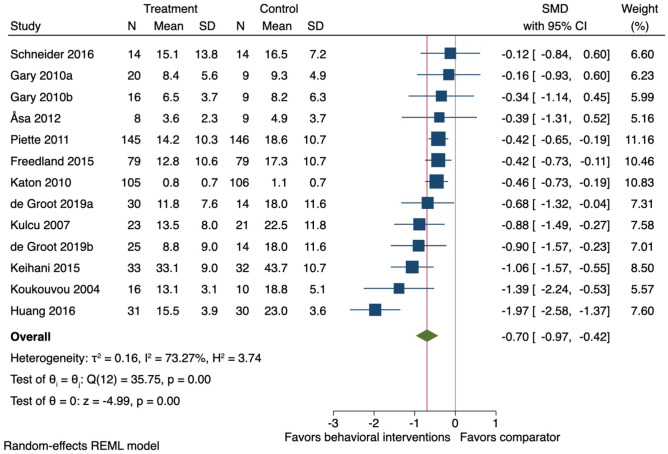
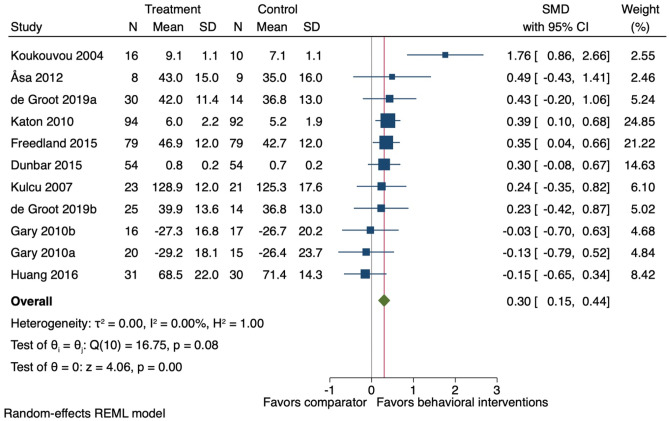
Results: Fourteen studies involving 1,378 people. Behavioural interventions had little to no effect on physical activity (standardised mean difference 0.38, 95% CI -0.12-0.87) and the effect on weight loss was uncertain (BMI mean difference -0.17, 95% CI -1.1-0.83) at the end-treatment follow-up. Small improvements were seen in health-related quality of life (SMD 0.29, 95% CI 0.17-0.42) and physical function (SMD 0.42, 95% CI 0.12-0.73), and moderate improvements were seen for depression symptoms (SMD -0.70, 95% CI -0.97-0.42). Studies using the BCTs 'action planning' and 'social support (practical)' reported greater physical activity and weight loss.
Conclusions: Behavioural interventions targeting lifestyle behaviours may improve health-related quality of life and physical function, and reduce depression, whereas little to no effect was achieved on physical activity and weight loss in people with multimorbidity. However, the evidence for physical activity and weight loss were of low quality and the end-treatment benefits diminished over time.
Keywords: Behavioural therapy; Disability; Function; Health; Multimorbidity; Physical activity.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures







References
-
- Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10(4):430-9. PMID: 21402176. 10.1016/j.arr.2011.03.003. - PubMed
-
- Menotti A, Mulder I, Nissinen A, Giampaoli S, Feskens EJM, Kromhout D. Prevalence of morbidity and multimorbidity in elderly male populations and their impact on 10-year all-cause mortality: the FINE study (Finland, Italy, Netherlands, Elderly). J Clin Epidemiol. 2001;54(7):680-6. PMID: WOS:000169512800005. 10.1016/S0895-4356(00)00368-1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
