

The Effect of Endogenous Cushing Syndrome on All-cause and Cause-specific Mortality
- PMID: 35486378
- PMCID: PMC9282270
- DOI: 10.1210/clinem/dgac265
The Effect of Endogenous Cushing Syndrome on All-cause and Cause-specific Mortality
Abstract
Objective: We aimed to perform a systematic review and meta-analysis of all-cause and cause-specific mortality of patients with benign endogenous Cushing syndrome (CS).
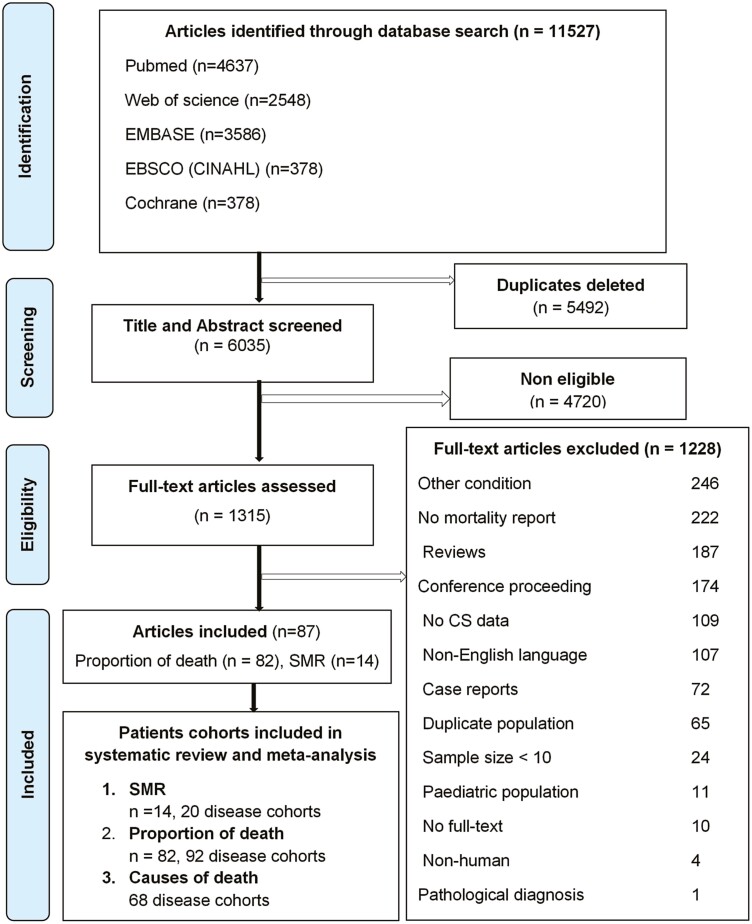
Methods: The protocol was registered in PROSPERO (CRD42017067530). PubMed, EMBASE, CINHAL, Web of Science, and Cochrane Central searches were undertaken from inception to January 2021. Outcomes were the standardized mortality ratio (SMR), proportion, and cause of deaths. The I2 test, subgroup analysis, and meta-regression were used to assess heterogeneity across studies.
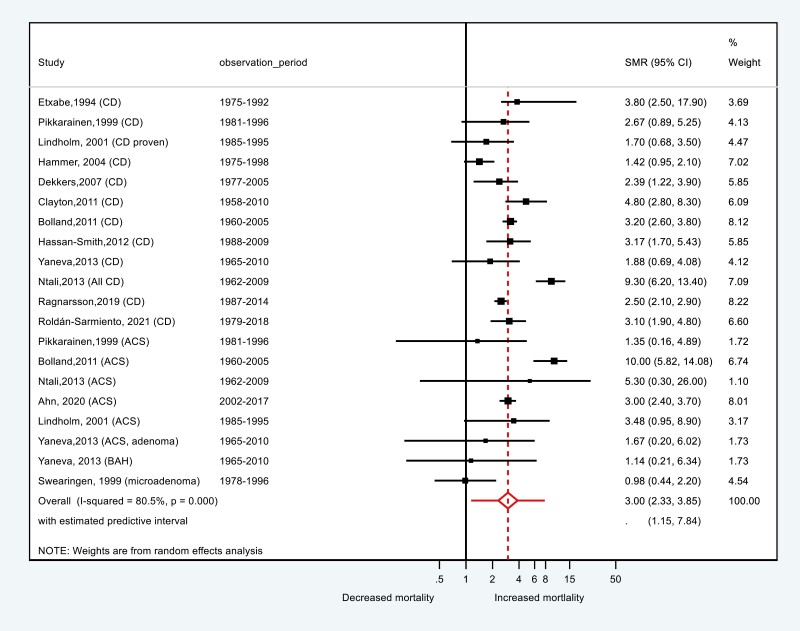
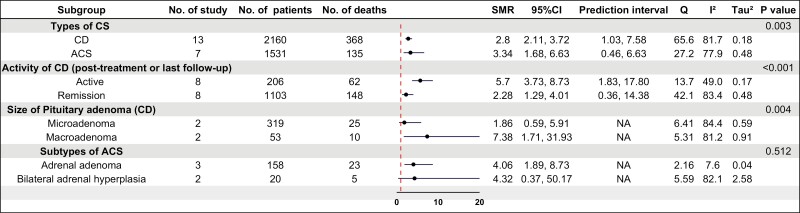
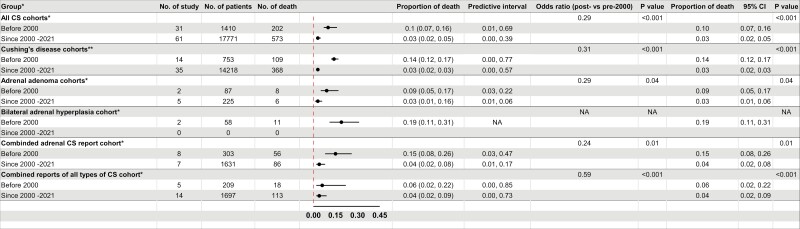
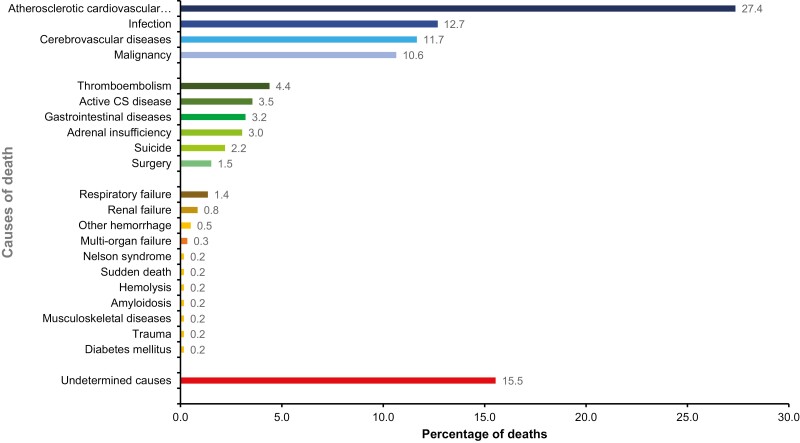
Results: SMR was reported in 14 articles including 3691 patients (13 Cushing disease [CD] and 7 adrenal CS [ACS] cohorts). Overall SMR was 3.0 (95% CI, 2.3-3.9; I2 = 80.5%) for all CS, 2.8 (95% CI, 2.1-3.7; I2 = 81.2%) for CD and 3.3 (95% CI, 0.5-6.6; I2 = 77.9%) for ACS. Proportion of deaths, reported in 87 articles including 19 181 CS patients (53 CD, 24 ACS, and 20 combined CS cohorts), was 0.05 (95% CI, 0.03-0.06) for all CS subtypes with meta-regression analysis revealing no differences between CS subtypes (P = .052). The proportion of deaths was 0.1 (10%) in articles published before 2000 and 0.03 (3%) in 2000 until the last search for CS (P < .001), CD (P < .001), and ACS (P = .01). The causes of death were atherosclerotic diseases and thromboembolism (43.4%), infection (12.7%), malignancy (10.6%), active disease (3.5%), adrenal insufficiency (3.0%), and suicide (2.2%). Despite improved outcomes in recent years, increased mortality from CS persists. The causes of death highlight the need to prevent and manage comorbidities in addition to treating hypercortisolism.
Keywords: Cushing syndrome; causes of death; meta-analysis; meta-regression analysis; mortality.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
Cushing Mortality in Remission: Not Out of the Woods.J Clin Endocrinol Metab. 2022 Sep 28;107(10):e4232-e4233. doi: 10.1210/clinem/dgac341. J Clin Endocrinol Metab. 2022. PMID: 35648700 Free PMC article. No abstract available.
References
-
- Hasenmajer V, Sbardella E, Sciarra F, Minnetti M, Isidori AM, Venneri MA. The immune system in Cushing’s syndrome. Trends Endocrinol Metab. 2020;31(9):655-669. - PubMed
-
- Etxabe J, Vazquez JA. Morbidity and mortality in Cushing’s disease: an epidemiological approach. Clin Endocrinol (Oxf). 1994;40(4):479-484. - PubMed
-
- Raappana A, Koivukangas J, Ebeling T, Pirilä T. Incidence of pituitary adenomas in Northern Finland in 1992-2007. J Clin Endocrinol Metab. 2010;95(9):4268-4275. - PubMed
-
- Boscaro M, Arnaldi G. Approach to the patient with possible Cushing’s syndrome. J Clin Endocrinol Metab. 2009;94(9):3121-3131. - PubMed
