

Association of Influenza Vaccination With Cardiovascular Risk: A Meta-analysis
- PMID: 35486404
- PMCID: PMC9055450
- DOI: 10.1001/jamanetworkopen.2022.8873
Association of Influenza Vaccination With Cardiovascular Risk: A Meta-analysis
Abstract
Importance: Influenza infection is associated with increased cardiovascular hospitalization and mortality. Our prior systematic review and meta-analysis hypothesized that influenza vaccination was associated with a lower risk of cardiovascular events.
Objective: To evaluate, via an updated meta-analysis, if seasonal influenza vaccination is associated with a lower risk of fatal and nonfatal cardiovascular events and assess whether the newest cardiovascular outcome trial results are consistent with prior findings.
Data sources: A previously published meta-analysis of randomized controlled trials (RCTs) and a large 2021 cardiovascular outcome trial.
Study selection: Studies with RCTs published between 2000 and 2021 that randomized participants to either influenza vaccine or placebo/control. Eligible participants were inpatients and outpatients recruited for international multicenter RCTs and randomized to receive either influenza vaccine or placebo/control.
Data extraction and synthesis: PRISMA guidelines were followed in the extraction of study details, and risk of bias was assessed using the Cochrane Collaboration tool. Trial quality was evaluated using Cochrane criteria. Data were analyzed January 2020 and December 2021.
Main outcomes and measures: Random-effects Mantel-Haenszel risk ratios (RRs) and 95% CIs were derived for a composite of major adverse cardiovascular events and cardiovascular mortality within 12 months of follow-up. Where available, analyses were stratified by patients with and without recent acute coronary syndrome (ACS) within 1 year of randomization.
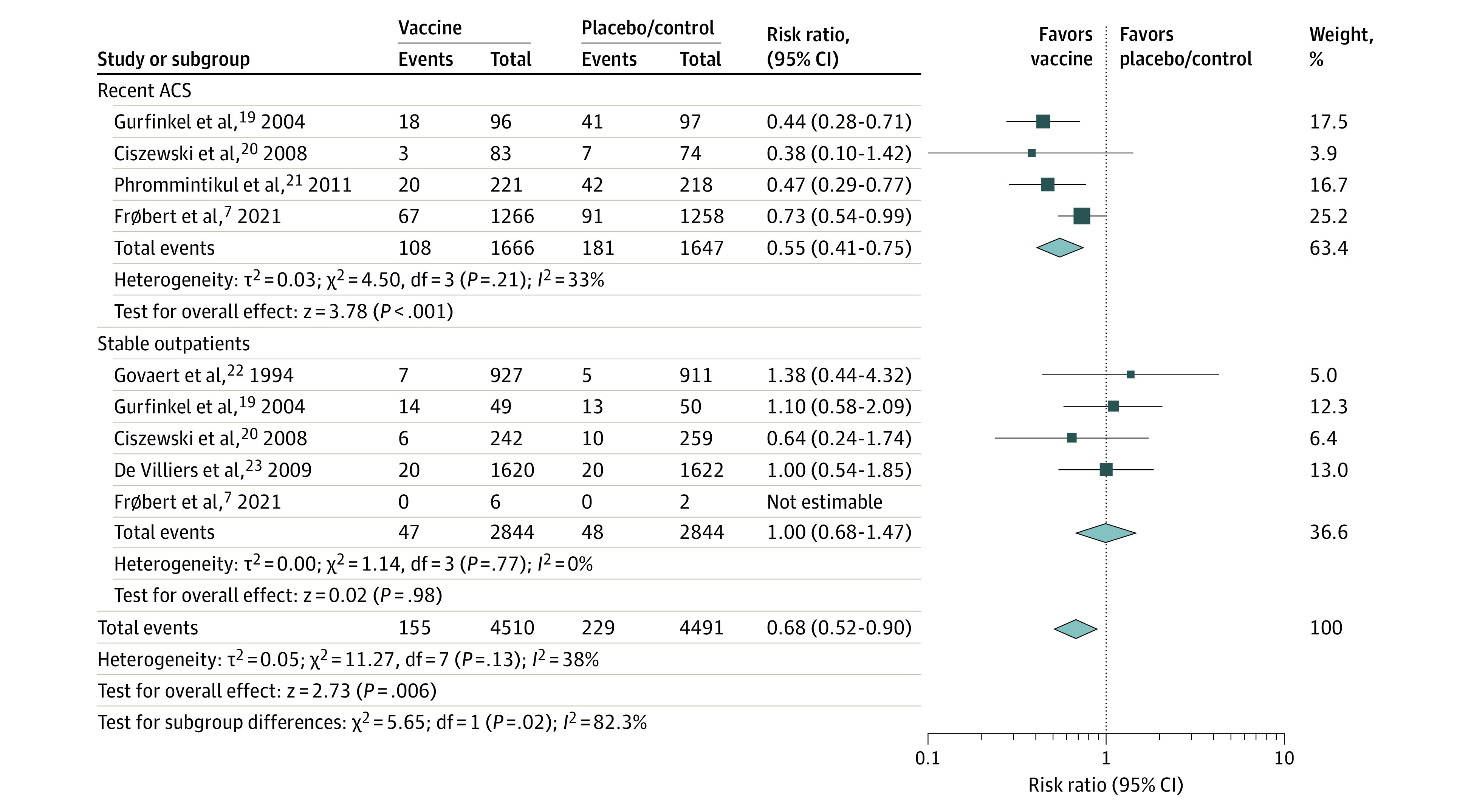
Results: Six published RCTs comprising a total of 9001 patients were included (mean age, 65.5 years; 42.5% women; 52.3% with a cardiac history). Overall, influenza vaccine was associated with a lower risk of composite cardiovascular events (3.6% vs 5.4%; RR, 0.66; 95% CI, 0.53-0.83; P < .001). A treatment interaction was detected between patients with recent ACS (RR, 0.55; 95% CI, 0.41-0.75) and without recent ACS (RR, 1.00; 95% CI, 0.68-1.47) (P for interaction = .02). For cardiovascular mortality, a treatment interaction was also detected between patients with recent ACS (RR, 0.44; 95% CI, 0.23-0.85) and without recent ACS (RR, 1.45; 95% CI, 0.84-2.50) (P for interaction = .006), while 1.7% of vaccine recipients died of cardiovascular causes compared with 2.5% of placebo or control recipients (RR, 0.74; 95% CI, 0.42-1.30; P = .29).
Conclusions and relevance: In this study, receipt of influenza vaccination was associated with a 34% lower risk of major adverse cardiovascular events, and individuals with recent ACS had a 45% lower risk. Given influenza poses a threat to population health during the COVID-19 pandemic, it is integral to counsel high-risk patients on the cardiovascular benefits of influenza vaccination.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
