

Overcoming differential tumor penetration of BRAF inhibitors using computationally guided combination therapy
- PMID: 35486732
- PMCID: PMC9054019
- DOI: 10.1126/sciadv.abl6339
Overcoming differential tumor penetration of BRAF inhibitors using computationally guided combination therapy
Abstract
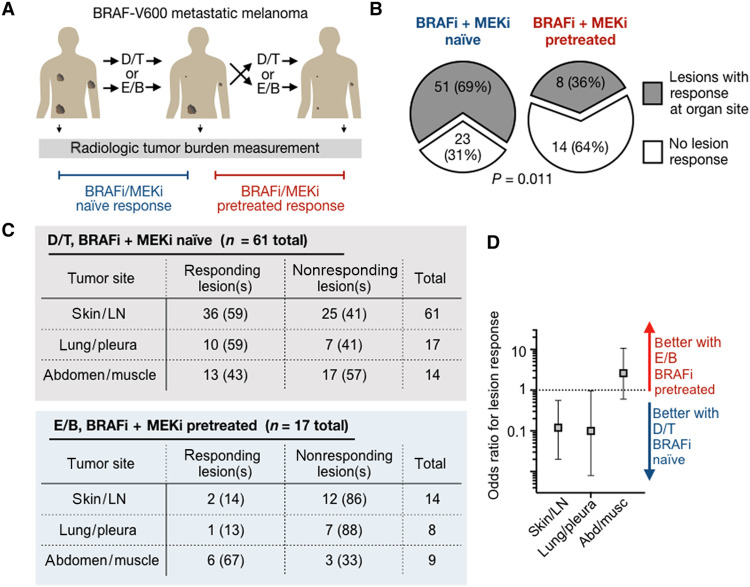
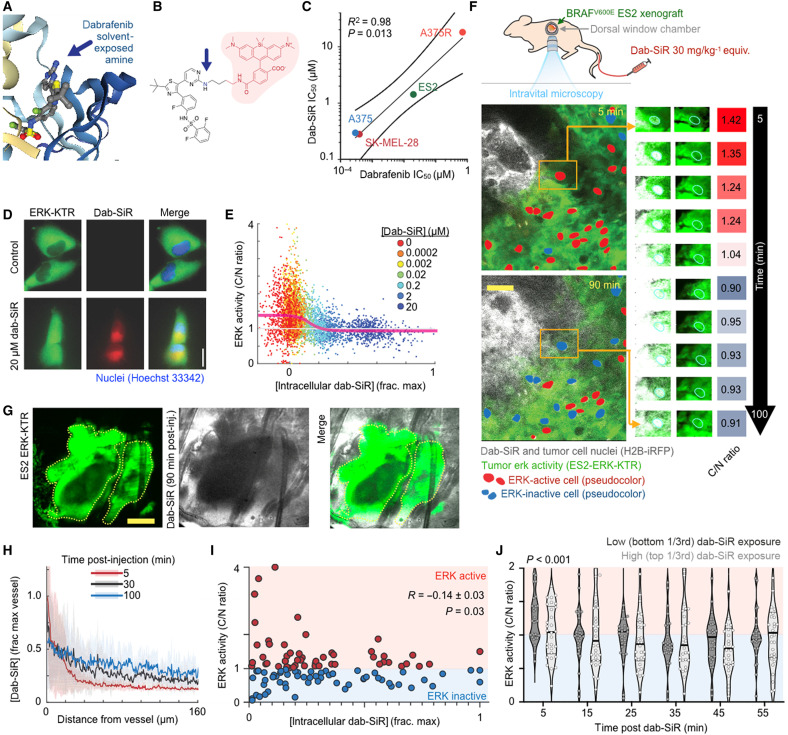
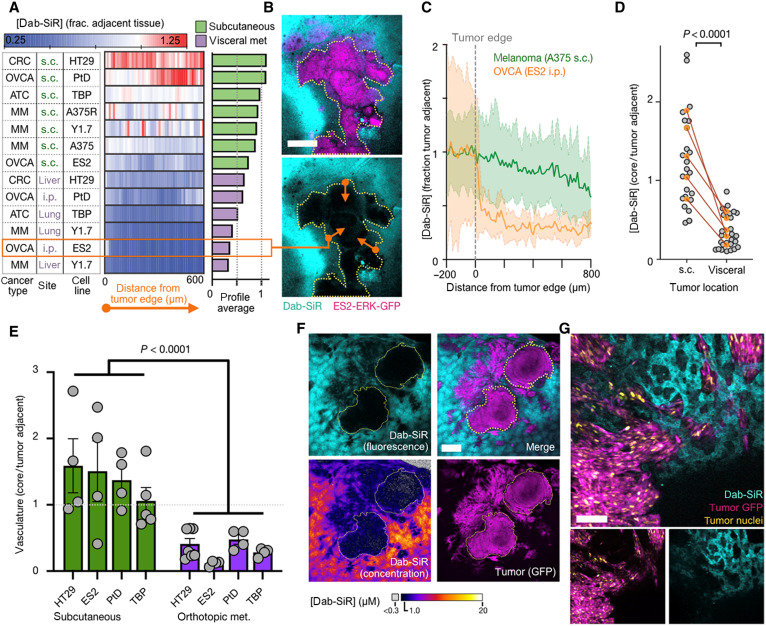
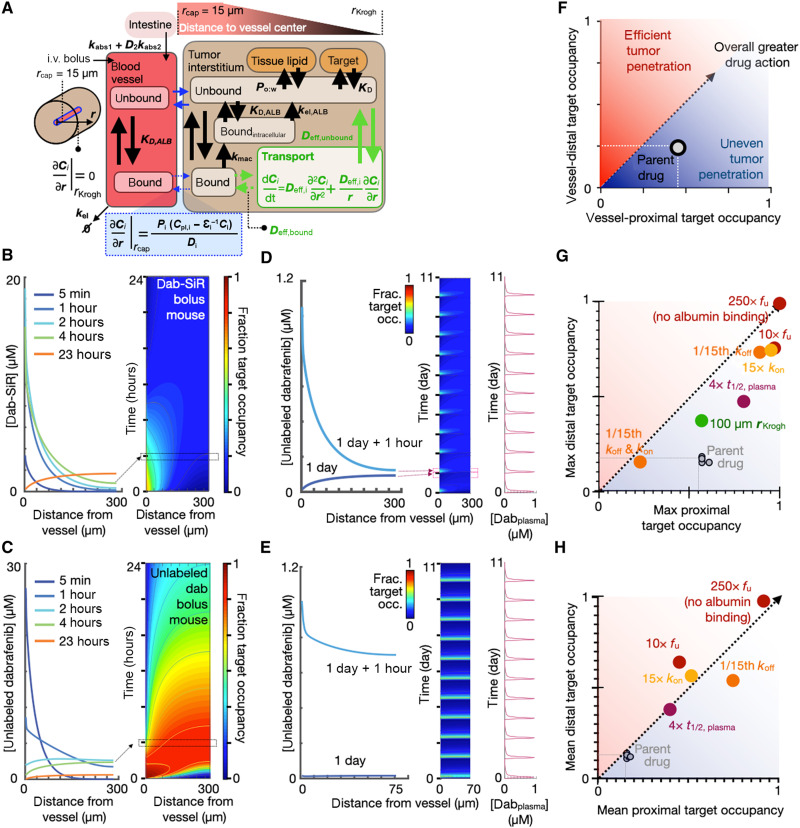
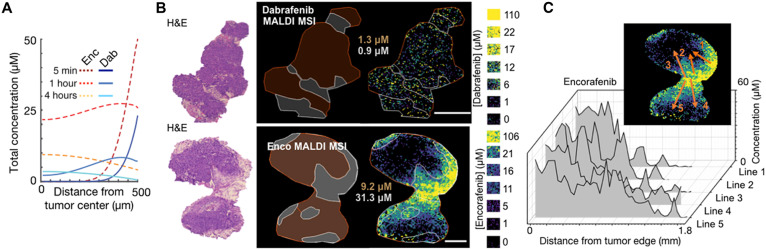
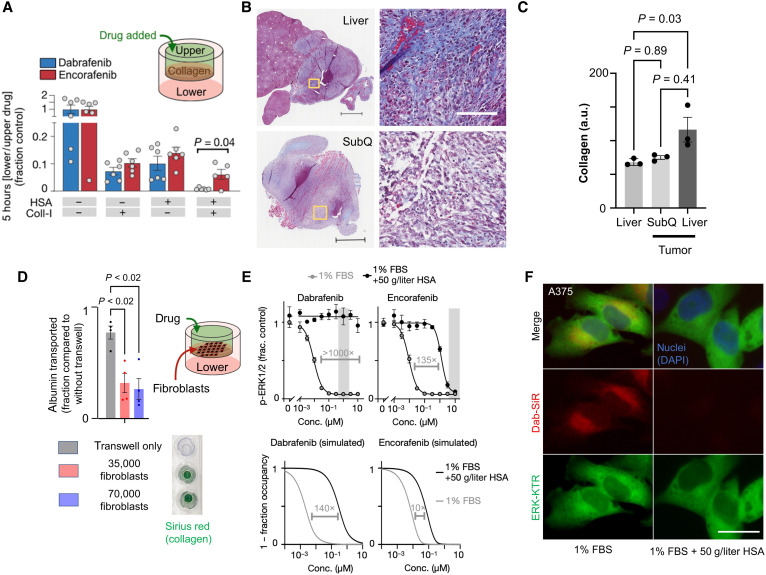
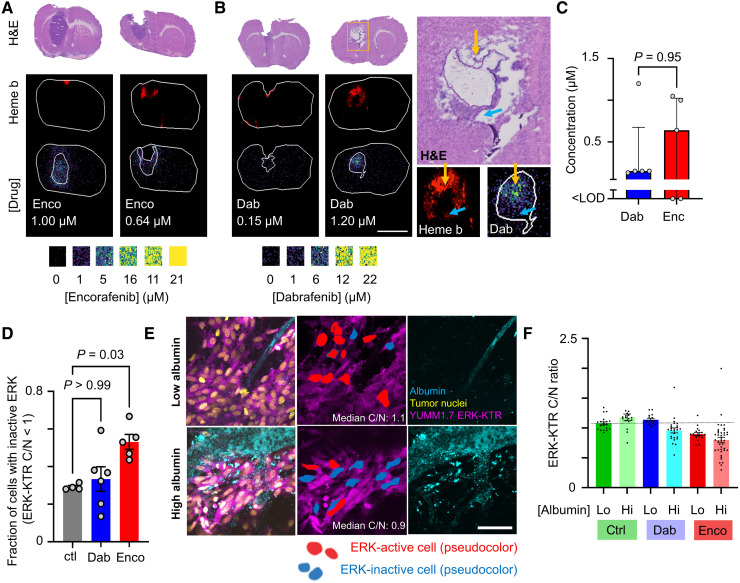
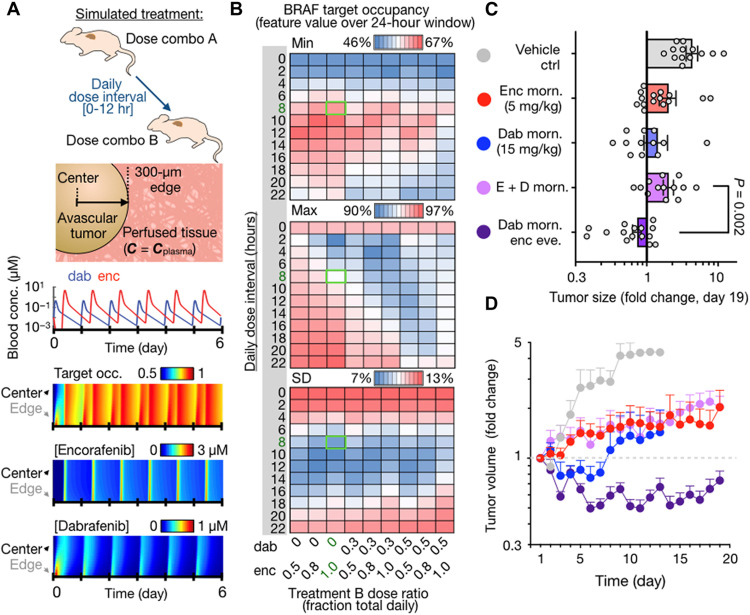
BRAF-targeted kinase inhibitors (KIs) are used to treat malignancies including BRAF-mutant non-small cell lung cancer, colorectal cancer, anaplastic thyroid cancer, and, most prominently, melanoma. However, KI selection criteria in patients remain unclear, as are pharmacokinetic/pharmacodynamic (PK/PD) mechanisms that may limit context-dependent efficacy and differentiate related drugs. To address this issue, we imaged mouse models of BRAF-mutant cancers, fluorescent KI tracers, and unlabeled drug to calibrate in silico spatial PK/PD models. Results indicated that drug lipophilicity, plasma clearance, faster target dissociation, and, in particular, high albumin binding could limit dabrafenib action in visceral metastases compared to other KIs. This correlated with retrospective clinical observations. Computational modeling identified a timed strategy for combining dabrafenib and encorafenib to better sustain BRAF inhibition, which showed enhanced efficacy in mice. This study thus offers principles of spatial drug action that may help guide drug development, KI selection, and combination.
Figures
References
-
- Delord J., Robert C., Nyakas M., McArthur G., Kudchakar R., Mahipal A., Yamada Y., Sullivan R., Arance A., Kefford R., Carlino M., Hidalgo M., Gomez-Roca C., Michel D., Seroutou A., Aslanis V., Caponigro G., Stuart D., Moutouh-de Parseval L., Demuth T., Dummer R., Phase I dose-escalation and -expansion study of the braf inhibitor encorafenib (LGX818) in metastatic BRAF-mutant melanoma. Clin. Cancer Res. 23, 5339–5348 (2017). - PubMed
-
- Subbiah V., Puzanov I., Blay J. Y., Chau I., Lockhart A. C., Raje N. S., Wolf J., Baselga J., Meric-Bernstam F., Roszik J., Diamond E. L., Riely G. J., Sherman E. J., Riehl T., Pitcher B., Hyman D. M., Pan-cancer efficacy of vemurafenib in BRAF (V600)-mutant non-melanoma cancers. Cancer Discov. 10, 657–663 (2020). - PMC - PubMed
-
- Corcoran R., André T., Atreya C., Schellens J., Yoshino T., Bendell J., Hollebecque A., McRee A., Siena S., Middleton G., Muro K., Gordon M., Tabernero J., Yaeger R., O’Dwyer P., Humblet Y., De Vos F., Jung A., Brase J., Jaeger S., Bettinger S., Mookerjee B., Rangwala F., Van Cutsem E., Combined BRAF, EGFR, and MEK inhibition in patients with BRAFV600E-mutant colorectal cancer. Cancer Discov. 8, 428–443 (2018). - PMC - PubMed
-
- Dummer R., Ascierto P., Gogas H., Arance A., Mandala M., Liszkay G., Garbe C., Schadendorf D., Krajsova I., Gutzmer R., Chiarion-Sileni V., Dutriaux C., de Groot J., Yamazaki N., Loquai C., Moutouh-de Parseval L., Pickard M., Sandor V., Robert C., Flaherty K., Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 19, 603–615 (2018). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
