

Travel of pregnant women in emergency situations to hospital and maternal mortality in Lagos, Nigeria: a retrospective cohort study
- PMID: 35487675
- PMCID: PMC9058694
- DOI: 10.1136/bmjgh-2022-008604
Travel of pregnant women in emergency situations to hospital and maternal mortality in Lagos, Nigeria: a retrospective cohort study
Abstract
Introduction: Prompt access to emergency obstetrical care (EmOC) reduces the risk of maternal mortality. We assessed institutional maternal mortality by distance and travel time for pregnant women with obstetrical emergencies in Lagos State, Nigeria.
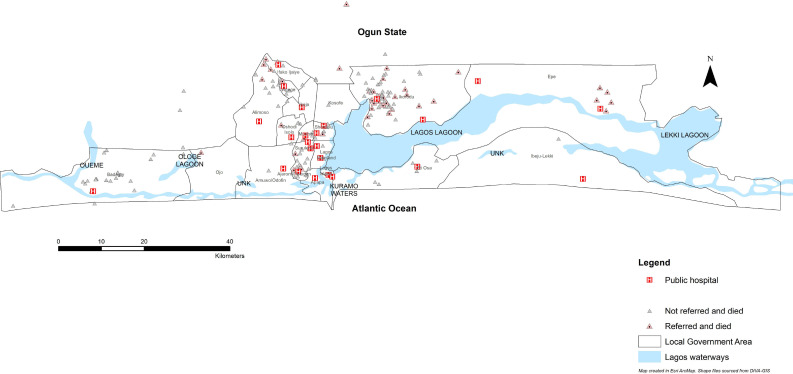
Methods: We conducted a facility-based retrospective cohort study across 24 public hospitals in Lagos. Reviewing case notes of the pregnant women presenting between 1 November 2018 and 30 October 2019, we extracted socio-demographic, travel and obstetrical data. The extracted travel data were exported to Google Maps, where driving distance and travel time data were extracted. Multivariable logistic regression was conducted to determine the relative influence of distance and travel time on maternal death.
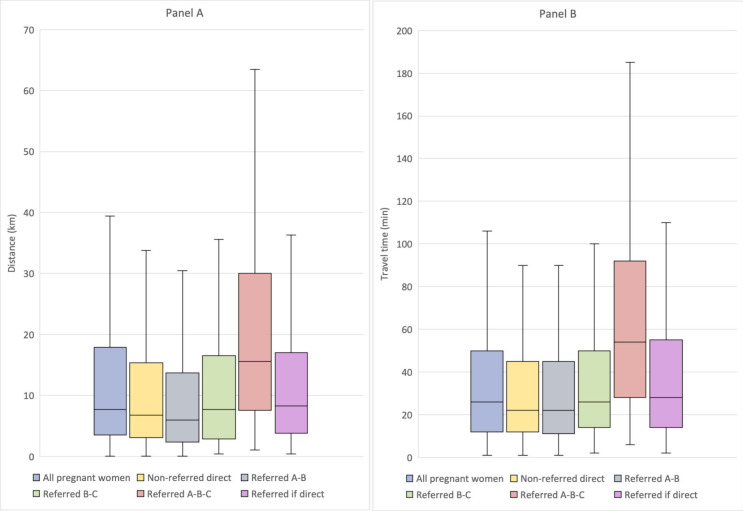
Findings: Of 4181 pregnant women with obstetrical emergencies, 182 (4.4%) resulted in maternal deaths. Among those who died, 60.3% travelled ≤10 km directly from home, and 61.9% arrived at the hospital ≤30 mins. The median distance and travel time to EmOC was 7.6 km (IQR 3.4-18.0) and 26 mins (IQR 12-50). For all women, travelling 10-15 km (2.53, 95% CI 1.27 to 5.03) was significantly associated with maternal death. Stratified by referral, odds remained statistically significant for those travelling 10-15 km in the non-referred group (2.48, 95% CI 1.18 to 5.23) and for travel ≥120 min (7.05, 95% CI 1.10 to 45.32). For those referred, odds became statistically significant at 25-35 km (21.40, 95% CI 1.24 to 36.72) and for journeys requiring travel time from as little as 10-29 min (184.23, 95% CI 5.14 to 608.51). Odds were also significantly higher for women travelling to hospitals in suburban (3.60, 95% CI 1.59 to 8.18) or rural (2.51, 95% CI 1.01 to 6.29) areas.
Conclusion: Our evidence shows that distance and travel time influence maternal mortality differently for referred women and those who are not. Larger scale research that uses closer-to-reality travel time and distance estimates as we have done, rethinking of global guidelines, and bold actions addressing access gaps, including within the suburbs, will be critical in reducing maternal mortality by 2030.
Keywords: health services research; hospital-based study; maternal health; obstetrics.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO, UNICEF, UNFPA, World Bank Group, UNDP . Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division [online]. Geneva: World Health Organization, 2019: 1–119. https://www.unfpa.org/sites/default/files/pub-pdf/Maternal_mortality_rep...
-
- UNICEF, WHO, World Bank, UNPD . A neglected tragedy: the global burden of stillbirths. New York: United Nations Children’s Fund, 2020: 1–90.
-
- United Nations . Sustainable development goals: 17 goals to transform our world [online]. Sustainable Development Goals, 2016. Available: http://www.un.org/sustainabledevelopment/sustainable-development-goals/ [Accessed 12 Oct 2020].
-
- WHO, UNFPA, UNICEF, Averting Maternal Deaths and Disabilities . Monitoring emergency obstetric care: a handbook. Geneva, Switzerland: WHO Press, 2009.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources