

Development of a Novel Emergency Department Quality Measure to Reduce Very Low-Risk Syncope Hospitalizations
- PMID: 35487840
- PMCID: PMC9117517
- DOI: 10.1016/j.annemergmed.2022.03.008
Development of a Novel Emergency Department Quality Measure to Reduce Very Low-Risk Syncope Hospitalizations
Abstract
Study objective: Emergency department (ED) evaluations for syncope are common, representing 1.3 million annual US visits and $2 billion in related hospitalizations. Despite evidence supporting risk stratification and outpatient management, variation in syncope hospitalization rates persist. We sought to develop a new quality measure for very low-risk adult ED patients with syncope that could be applied to administrative data.
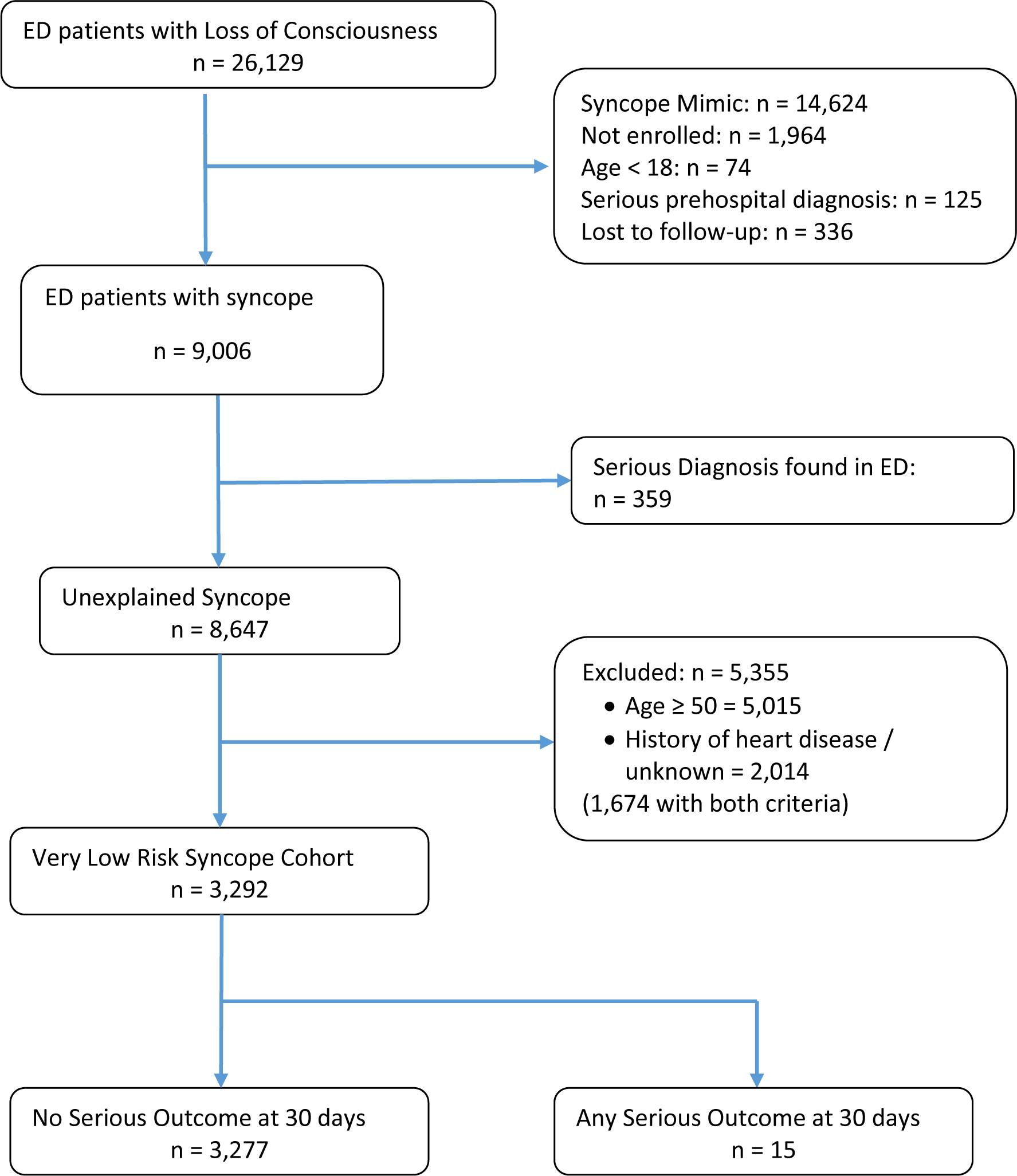
Methods: We developed this quality measure in 2 phases. First, we used an existing prospective, observational ED patient data set to identify a very low-risk cohort with unexplained syncope using 2 variables: age less than 50 years and no history of heart disease. We then applied this to the 2019 Nationwide Emergency Department Sample (NEDS) to assess its potential effect, assessing for hospital-level factors associated with hospitalization variation.
Results: Of the 8,647 adult patients in the prospective cohort, 3,292 (38%) patients fulfilled these 2 criteria: age less than 50 years and no history of heart disease. Of these, 15 (0.46%) suffered serious adverse events within 30 days. In the NEDS, there were an estimated 566,031 patients meeting these 2 criteria, of whom 15,507 (2.7%; 95% confidence interval [CI] 2.48% to 3.00%) were hospitalized. We found substantial variation in the hospitalization rates for this very low-risk cohort, with a median rate of 1.7% (range 0% to 100%; interquartile range 0% to 3.9%). Factors associated with increased hospitalization rates included a yearly ED volume of more than 80,000 (odds ratio [OR] 3.14; 95% CI 2.02 to 4.89) and metropolitan teaching status (OR 1.5; 95% CI 1.24 to 1.81).
Conclusion: In summary, our novel syncope quality measure can assess variation in low-value hospitalizations for unexplained syncope. The application of this measure could improve the value of syncope care.
Copyright © 2022 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- Sun BC, Emond JA, Camargo CA Jr. Direct medical costs of syncope-related hospitalizations in the United States. The American journal of cardiology. 2005;95(5):668–671. - PubMed
-
- Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Development of the Canadian Syncope Risk Score to predict serious adverse events after emergency department assessment of syncope. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 2016;188(12):E289–298. - PMC - PubMed
-
- Quinn JV, Stiell IG, McDermott DA, Sellers KL, Kohn MA, Wells GA. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Annals of emergency medicine. 2004;43(2):224–232. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
