

Evaluation of CSTB and DMBT1 expression in saliva of gastric cancer patients and controls
- PMID: 35488257
- PMCID: PMC9055774
- DOI: 10.1186/s12885-022-09570-9
Evaluation of CSTB and DMBT1 expression in saliva of gastric cancer patients and controls
Abstract
Background: Gastric cancer (GC) is the fifth most common cancer and the third cause of cancer deaths globally, with late diagnosis, low survival rate, and poor prognosis. This case-control study aimed to evaluate the expression of cystatin B (CSTB) and deleted in malignant brain tumor 1 (DMBT1) in the saliva of GC patients with healthy individuals to construct diagnostic algorithms using statistical analysis and machine learning methods.
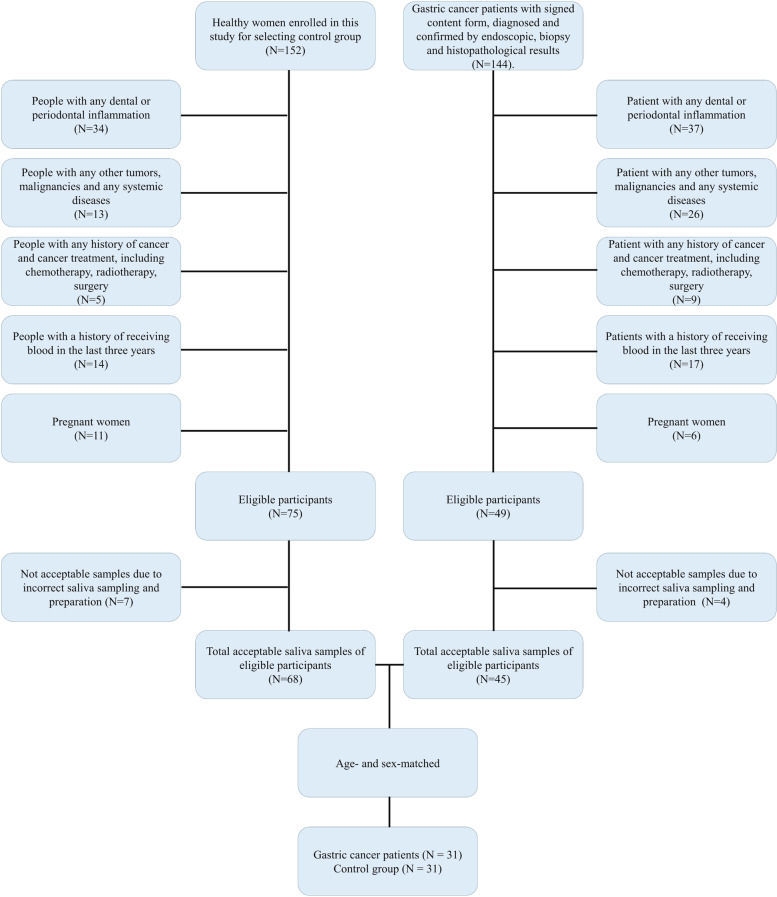
Methods: Demographic data, clinical characteristics, and food intake habits of the case and control group were gathered through a standard checklist. Unstimulated whole saliva samples were taken from 31 healthy individuals and 31 GC patients. Through ELISA test and statistical analysis, the expression of salivary CSTB and DMBT1 proteins was evaluated. To construct diagnostic algorithms, we used the machine learning method.
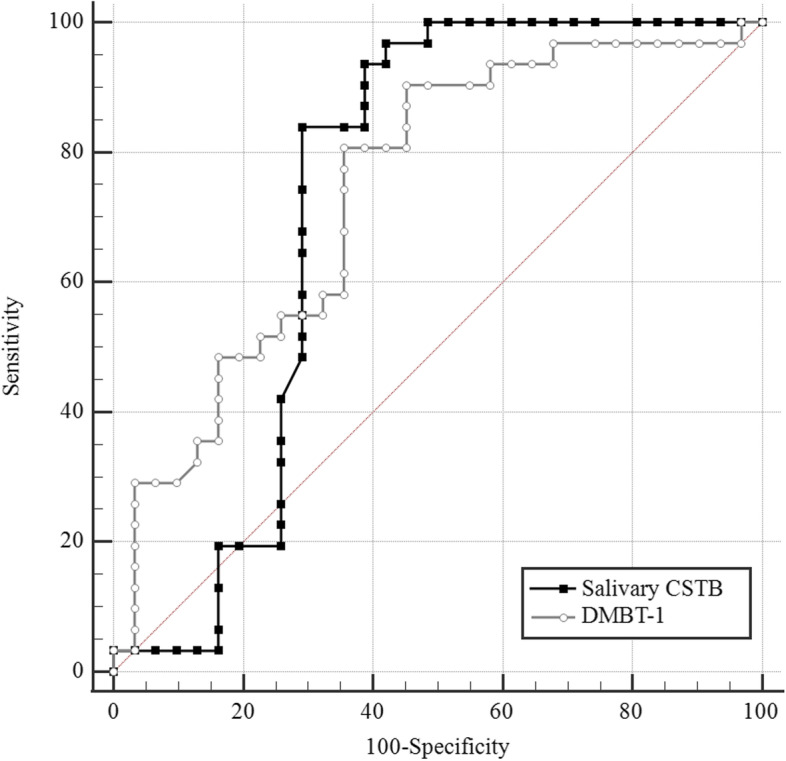
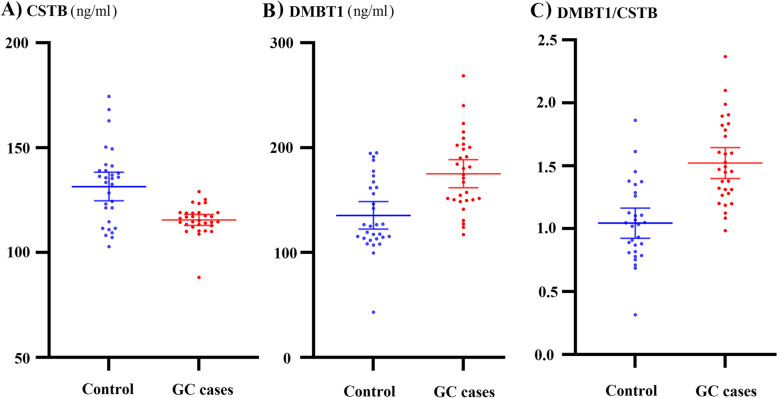
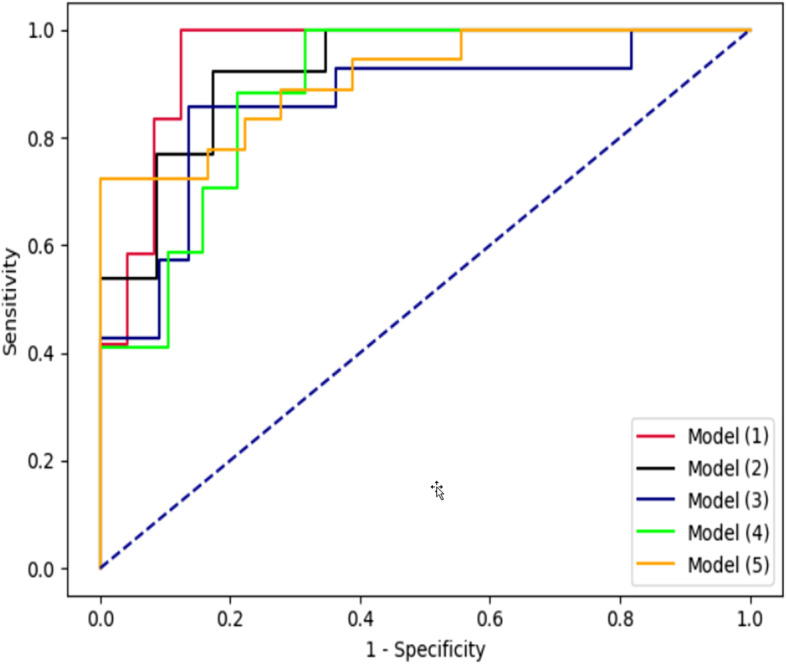
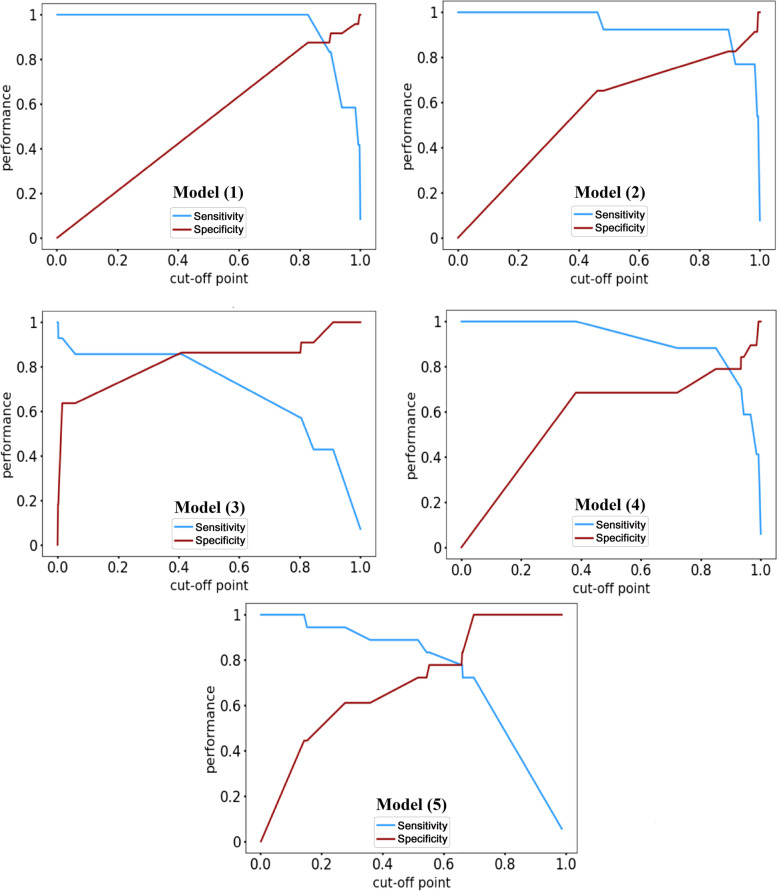
Results: The mean salivary expression of CSTB in GC patients was significantly lower (115.55 ± 7.06, p = 0.001), and the mean salivary expression of DMBT1 in GC patients was significantly higher (171.88 ± 39.67, p = 0.002) than the control. Multiple linear regression analysis demonstrated that GC was significantly correlated with high levels of DMBT1 after controlling the effects of age of participants (R2 = 0.20, p < 0.001). Considering salivary CSTB greater than 119.06 ng/mL as an optimal cut-off value, the sensitivity and specificity of CSTB in the diagnosis of GC were 83.87 and 70.97%, respectively. The area under the ROC curve was calculated as 0.728. The optimal cut-off value of DMBT1 for differentiating GC patients from controls was greater than 146.33 ng/mL (sensitivity = 80.65% and specificity = 64.52%). The area under the ROC curve was up to 0.741. As a result of the machine learning method, the area under the receiver-operating characteristic curve for the diagnostic ability of CSTB, DMBT1, demographic data, clinical characteristics, and food intake habits was 0.95. The machine learning model's sensitivity, specificity, and accuracy were 100, 70.8, and 80.5%, respectively.
Conclusion: Salivary levels of DMBT1 and CSTB may be accurate in diagnosing GCs. Machine learning analyses using salivary biomarkers, demographic, clinical, and nutrition habits data simultaneously could provide affordability models with acceptable accuracy for differentiation of GC by a cost-effective and non-invasive method.
Keywords: CSTB; DMBT1; Gastric cancer; Machine learning; Saliva.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Expression of Salivary miRNAs, Clinical, and Demographic Features in the Early Detection of Gastric Cancer: A Statistical and Machine Learning Analysis.J Gastrointest Cancer. 2024 Nov 9;56(1):15. doi: 10.1007/s12029-024-01136-1. J Gastrointest Cancer. 2024. PMID: 39520622
-
Differential Proteomic Analysis of Human Saliva using Tandem Mass Tags Quantification for Gastric Cancer Detection.Sci Rep. 2016 Feb 25;6:22165. doi: 10.1038/srep22165. Sci Rep. 2016. PMID: 26911362 Free PMC article.
-
Salivary cystatin S levels in children with early childhood caries in comparison with caries-free children; statistical analysis and machine learning.BMC Oral Health. 2021 Dec 18;21(1):650. doi: 10.1186/s12903-021-02016-x. BMC Oral Health. 2021. PMID: 34922509 Free PMC article.
-
Reg3A (regenerating family member 3 alpha) acts as a tumor suppressor by targeting DMBT1 (deleted in malignant brain tumors 1) in gastric cancer.Bioengineered. 2021 Dec;12(1):7644-7655. doi: 10.1080/21655979.2021.1981800. Bioengineered. 2021. PMID: 34605357 Free PMC article.
-
Salivary biomarkers for the diagnosis of gastric cancer: a systematic review.Rev Cient Odontol (Lima). 2024 Jun 27;12(2):e199. doi: 10.21142/2523-2754-1202-2024-199. eCollection 2024 Apr-Jun. Rev Cient Odontol (Lima). 2024. PMID: 39119128 Free PMC article. Review.
Cited by
-
Comparison between Machine Learning and Multiple Linear Regression to Identify Abnormal Thallium Myocardial Perfusion Scan in Chinese Type 2 Diabetes.Diagnostics (Basel). 2022 Jul 3;12(7):1619. doi: 10.3390/diagnostics12071619. Diagnostics (Basel). 2022. PMID: 35885524 Free PMC article.
-
Gastric cancer detection by non-blood-based liquid biopsies: A systematic review looking into the last decade of research.United European Gastroenterol J. 2023 Feb;11(1):114-130. doi: 10.1002/ueg2.12328. Epub 2022 Dec 3. United European Gastroenterol J. 2023. PMID: 36461757 Free PMC article.
-
Comparison between multiple logistic regression and machine learning methods in prediction of abnormal thallium scans in type 2 diabetes.World J Clin Cases. 2023 Nov 26;11(33):7951-7964. doi: 10.12998/wjcc.v11.i33.7951. World J Clin Cases. 2023. PMID: 38075576 Free PMC article.
-
Multi-faceted attributes of salivary cell-free DNA as liquid biopsy biomarkers for gastric cancer detection.Biomark Res. 2023 Oct 10;11(1):90. doi: 10.1186/s40364-023-00524-2. Biomark Res. 2023. PMID: 37817261 Free PMC article.
-
B-cell specific Moloney murine leukemia virus insertion site 1 contributes to invasion, metastasis, and poor prognosis in salivary adenoid cystic carcinoma.J Dent Sci. 2024 Jan;19(1):21-31. doi: 10.1016/j.jds.2023.06.014. Epub 2023 Jun 24. J Dent Sci. 2024. PMID: 38303897 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
