

Early versus delay oral feeding for patients after upper gastrointestinal surgery: a systematic review and meta-analysis of randomized controlled trials
- PMID: 35488274
- PMCID: PMC9052660
- DOI: 10.1186/s12935-022-02586-y
Early versus delay oral feeding for patients after upper gastrointestinal surgery: a systematic review and meta-analysis of randomized controlled trials
Abstract
Purpose: To evaluate the efficacy and safety of early oral feeding (EOF) in patients after upper gastrointestinal surgery through meta-analysis of randomized controlled trials (RCTs).
Methods: We analyzed the endpoints of patients including the length of stay (LOS), time of first exhaust, anastomotic leakage and pneumonia from included studies. And we retrieved RCTs from medical literature databases. Weighted mean difference (WMD), risk ratios (RR) and 95% confidence intervals (CI) were calculated to compare the endpoints.
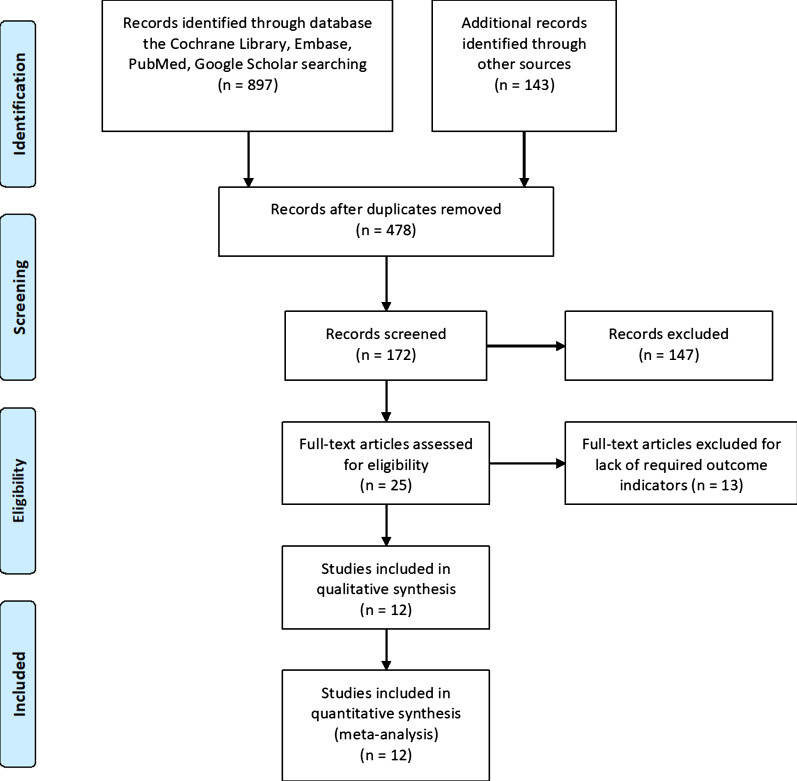
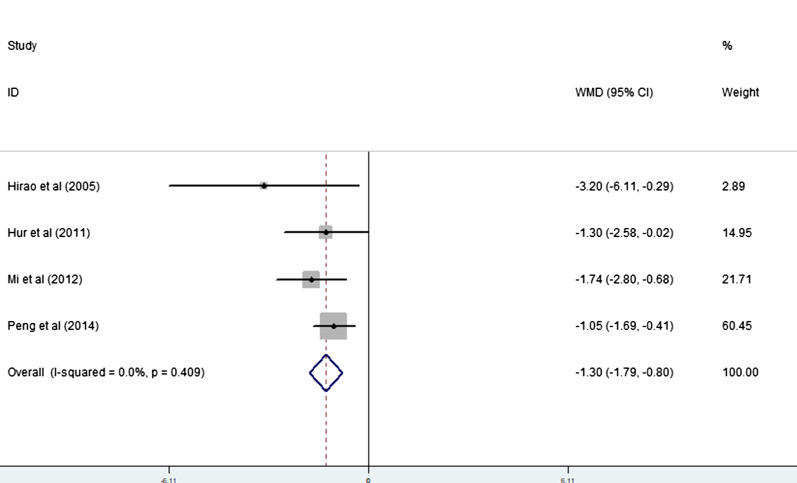
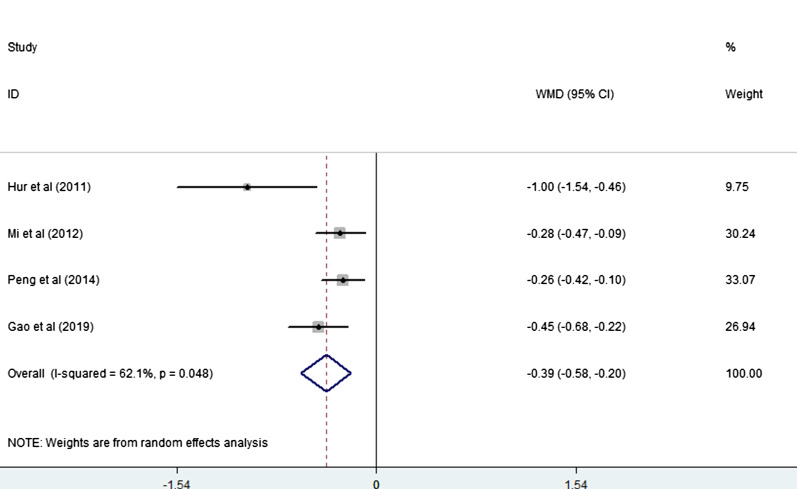
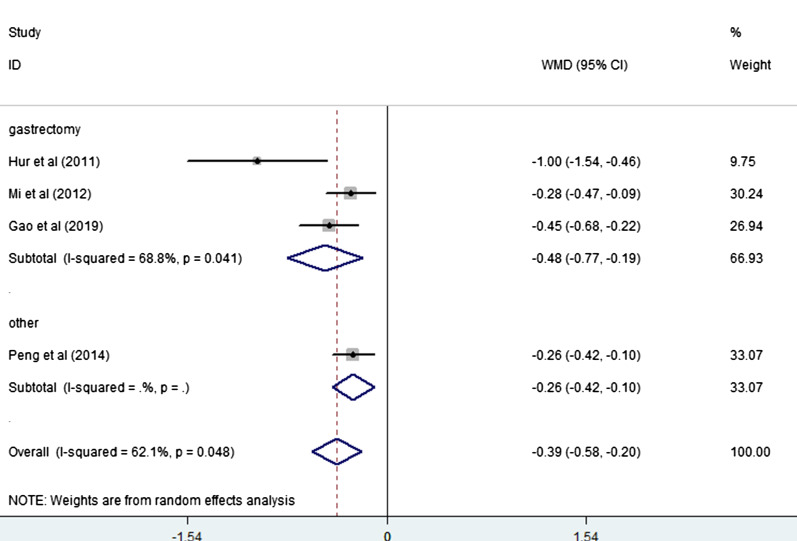
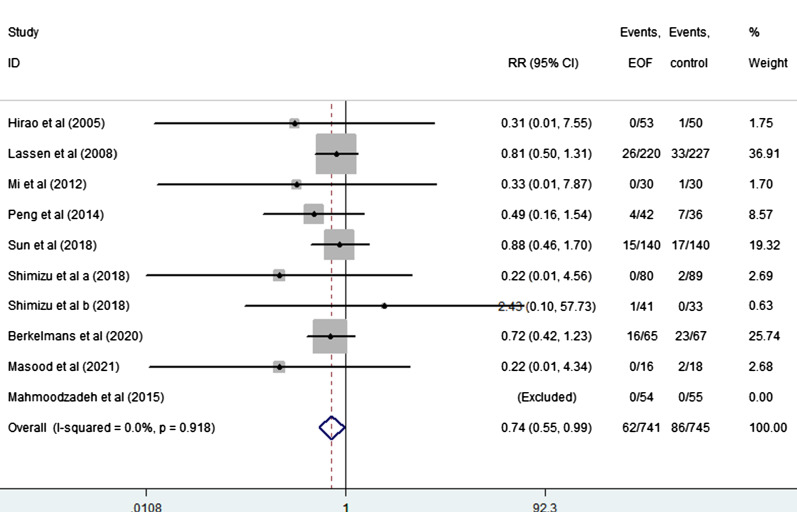
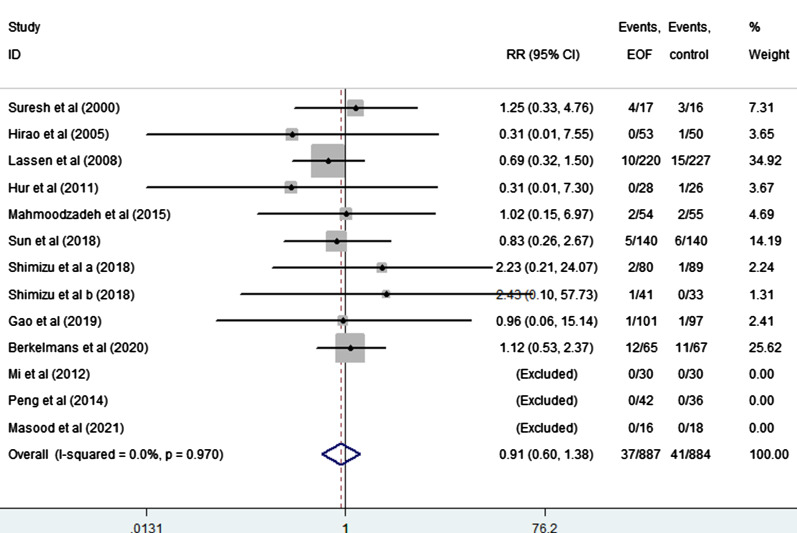
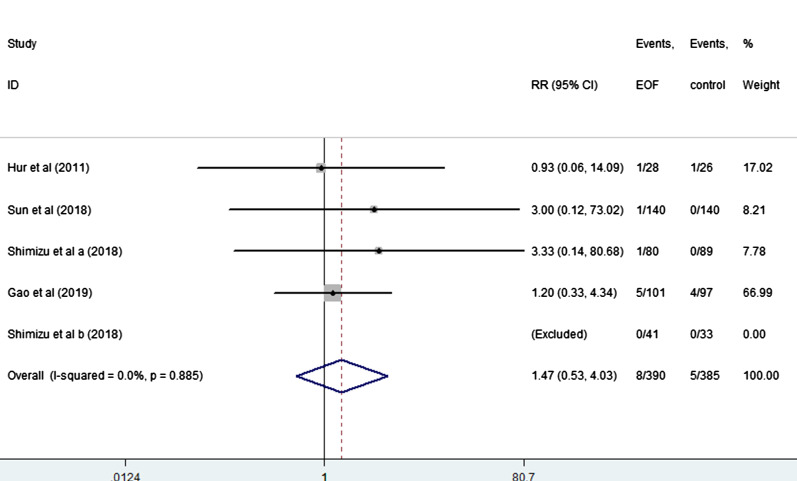
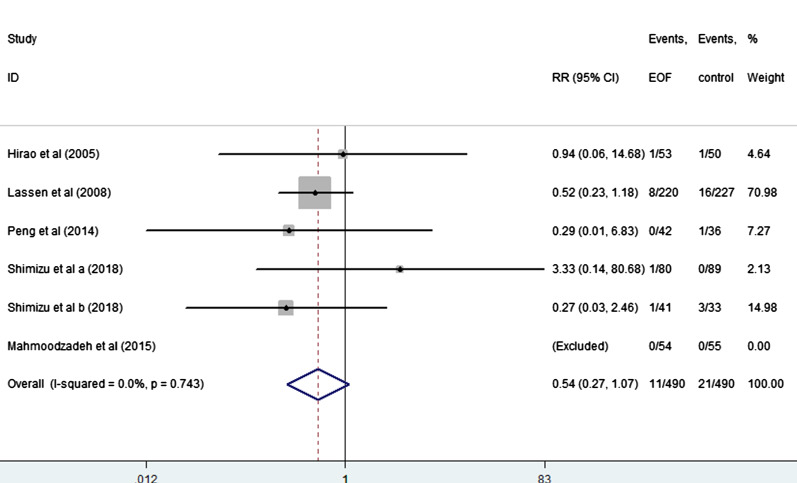
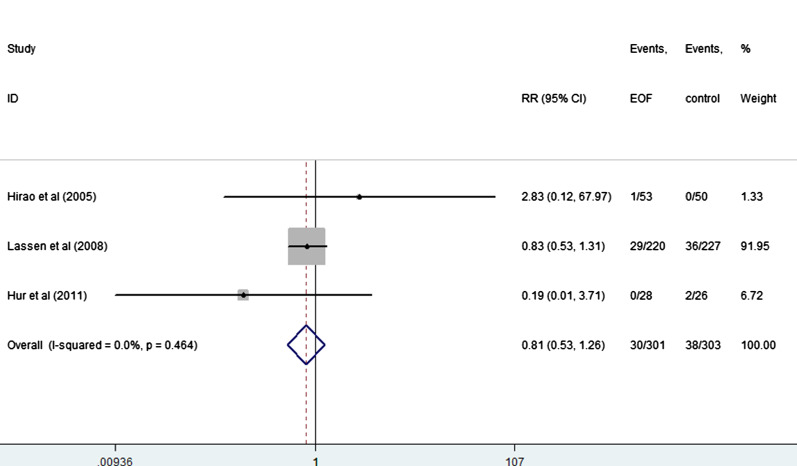
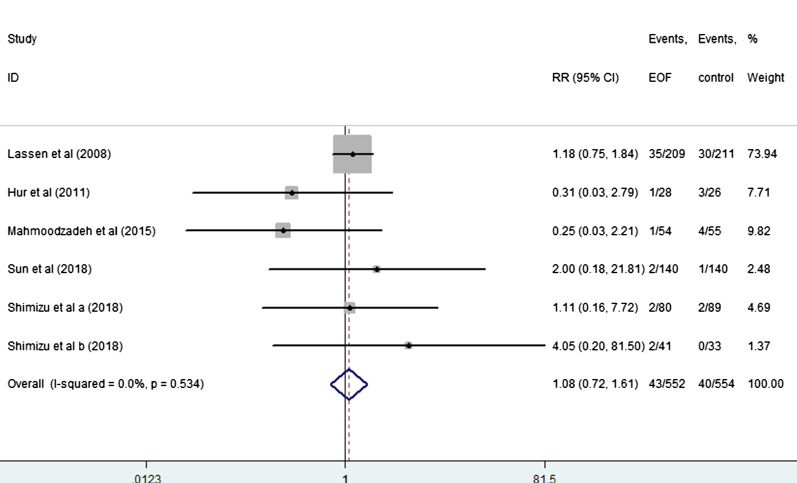
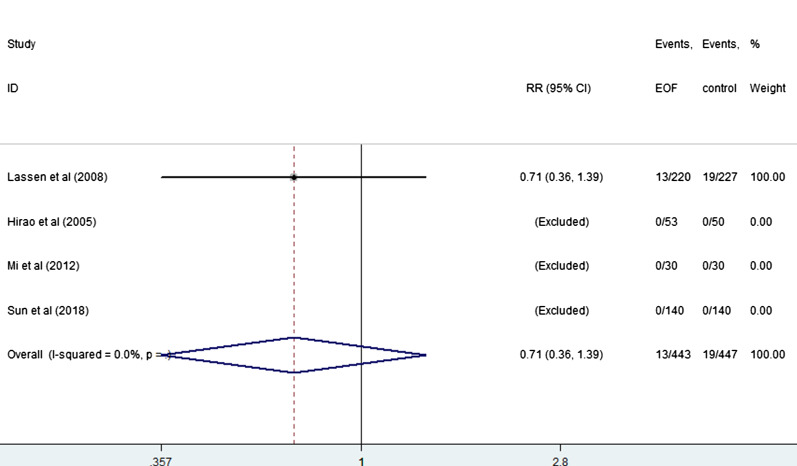
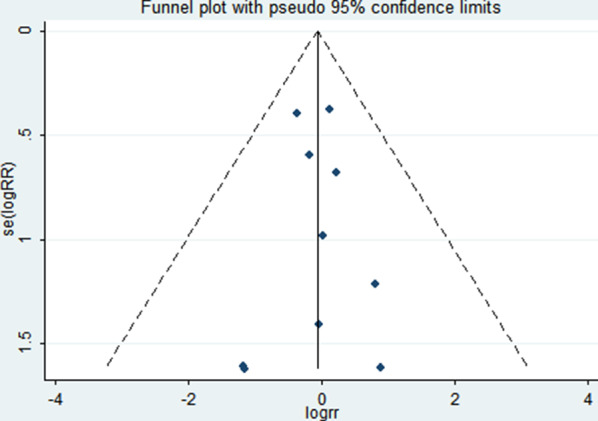
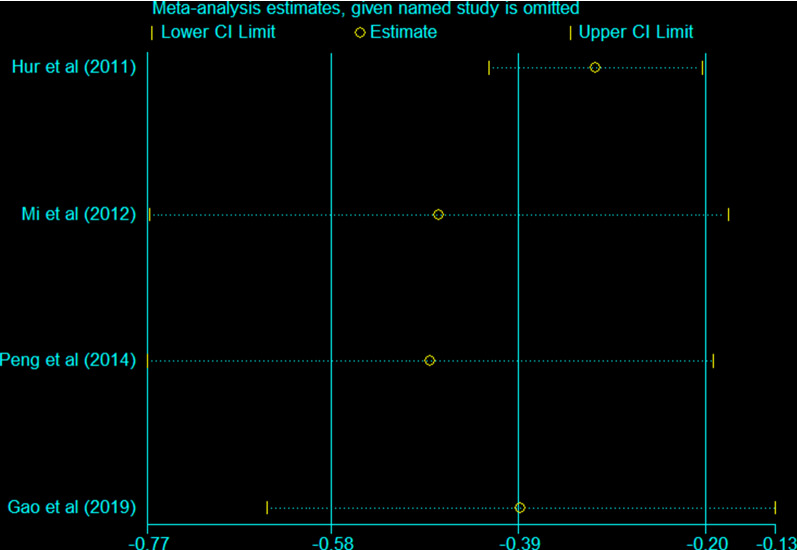
Results: In total, we retrieved 12 articles (13 trial comparisons) which contained 1771 patients. 887 patients (50.1%) were randomized to EOF group whereas 884 patients (49.9%) were randomized to delay oral feeding group. The result showed that compared with the delay oral feeding group, EOF after upper gastrointestinal surgery significantly shorten the LOS [WMD = - 1.30, 95% CI - 1.79 to - 0.80, I2 = 0.0%] and time of first exhaust [WMD = - 0.39, 95% CI - 0.58 to - 0.20, I2 = 62.1%]. EOF also reduced the risk of pneumonia (RR: 0.74, 95% CI 0.55 to 0.99, I2 = 0.0%). There is no significant difference in the risk of anastomotic leak, anastomotic bleeding, abdominal abscess, reoperation, readmission and mortality.
Conclusions: Overall, compared with the traditional oral feeding, EOF could shorten the LOS and time of first exhaust without increasing complications after upper gastrointestinal surgery.
Keywords: Early oral feeding; Meta-analysis; Upper gastrointestinal surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Figures
References
-
- Ishida Y, Inaba K, Suda K, et al. Upper gastrointestinal surgery on the esophagus and stomach. Nihon Geka Gakkai Zasshi. 2015;116:292–6. - PubMed
-
- Ye RC, Yun JH, Choi SH, et al. Effect of early enteral nutrition on the incidence of acute acalculous cholecystitis among trauma patients. Asia Pac J Clin Nutr. 2020;29(1):35–40. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
