

Predictive value of chromosome 18q11.2-q12.1 loss for benefit from bevacizumab in metastatic colorectal cancer: A post hoc analysis of the randomized phase III-trial AGITG-MAX
- PMID: 35489024
- PMCID: PMC9545440
- DOI: 10.1002/ijc.34061
Predictive value of chromosome 18q11.2-q12.1 loss for benefit from bevacizumab in metastatic colorectal cancer: A post hoc analysis of the randomized phase III-trial AGITG-MAX
Abstract
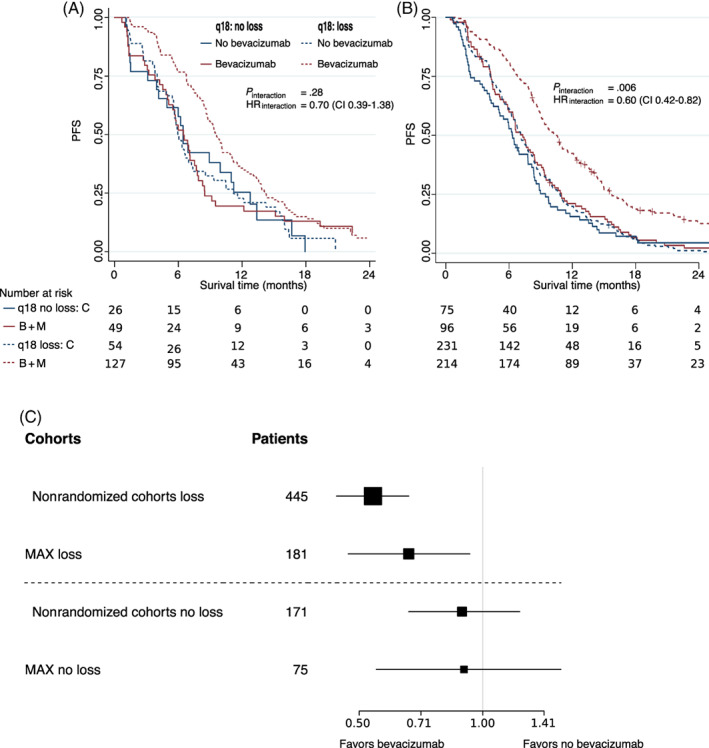
The VEGF-A monoclonal antibody bevacizumab is currently recommended for first-line treatment of all metastatic colorectal cancer (mCRC) patients. Cost-benefit ratio and side-effects however necessitate patient selection. A large retrospective yet nonrandomized study showed that patients with loss of chromosome 18q11.2-q12.1 in the tumor and treated with bevacizumab have 3 months improved median progression-free (PFS) and overall survival (OS) benefit compared to patients without this loss and/or treatment modality. Implementation for loss of chromosome 18q11.2-q12.1 as a marker in clinical practice mandates evidence in a randomized controlled trial for bevacizumab. Of the trials with randomization of chemotherapy vs chemotherapy with bevacizumab, the AGITG-MAX trial was the only one with tumor materials available. Chromosome 18q11.2-q12.1 copy number status was measured for 256 AGITG-MAX trial patients and correlated with PFS according to a predefined analysis plan with marker-treatment interaction as the primary end-point. Chromosome 18q11.2-q12.1 losses were detected in 71% of patients (181/256) characteristic for mCRC. Consistent with the nonrandomized study, significant PFS benefit of bevacizumab was observed in patients with chromosome 18q11.2-q12.1 loss (P = .009), and not in patients without 18q loss (P = .67). Although significance for marker-treatment interaction was not reached (Pinteraction = .28), hazard ratio and 95% confidence interval of this randomized cohort (HRinteraction = 0.72; 95% CI = 0.39-1.32) shows striking overlap with the nonrandomized study cohorts (HRinteraction = 0.41; 95% CI = 0.32-0.8) supported by a nonsignificant Cochrane χ2 test (P = .11) for heterogeneity. We conclude that post hoc analysis of the AGITG-MAX RCT provides supportive evidence for chromosome 18q11.2-q12.1 as a predictive marker for bevacizumab in mCRC patients.
Keywords: anti-VEGF monoclonal antibody; bevacizumab; chromosome 18q; metastatic colorectal cancer; predictive biomarker; randomized controlled trial.
© 2022 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Loss of Chromosome 18q11.2-q12.1 Is Predictive for Survival in Patients With Metastatic Colorectal Cancer Treated With Bevacizumab.J Clin Oncol. 2018 Jul 10;36(20):2052-2060. doi: 10.1200/JCO.2017.77.1782. Epub 2018 May 24. J Clin Oncol. 2018. PMID: 29792754 Clinical Trial.
-
The prognostic impact of consensus molecular subtypes (CMS) and its predictive effects for bevacizumab benefit in metastatic colorectal cancer: molecular analysis of the AGITG MAX clinical trial.Ann Oncol. 2018 Nov 1;29(11):2240-2246. doi: 10.1093/annonc/mdy410. Ann Oncol. 2018. PMID: 30247524 Clinical Trial.
-
Right or Left Primary Site of Colorectal Cancer: Outcomes From the Molecular Analysis of the AGITG MAX Trial.Clin Colorectal Cancer. 2019 Jun;18(2):141-148. doi: 10.1016/j.clcc.2018.12.002. Epub 2019 Jan 3. Clin Colorectal Cancer. 2019. PMID: 30713134
-
Monoclonal antibodies in the treatment of metastatic colorectal cancer: a review.Clin Ther. 2010 Mar;32(3):437-53. doi: 10.1016/j.clinthera.2010.03.012. Clin Ther. 2010. PMID: 20399983 Review.
-
Bevacizumab in combination with fluoropyrimidine-based chemotherapy for the first-line treatment of metastatic colorectal cancer.Health Technol Assess. 2010 Oct;14(Suppl. 2):47-53. doi: 10.3310/hta14suppl2/07. Health Technol Assess. 2010. PMID: 21047491 Review.
References
-
- Van Cutsem E, Cervantes A, Adam R, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27(8):1386‐1422. - PubMed
-
- Di Nicolantonio F, Vitiello PP, Marsoni S, et al. Precision oncology in metastatic colorectal cancer: from biology to medicine. Nat Rev Clin Oncol. 2021;2021(18):506‐525. - PubMed
-
- Baraniskin A, Buchberger B, Pox C, et al. Efficacy of bevacizumab in first‐line treatment of metastatic colorectal cancer: a systematic review and meta‐analysis. Eur J Cancer. 2019;106:37‐44. - PubMed
-
- Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350(23):2335‐2342. - PubMed
-
- Saltz LB, Clarke S, Díaz‐Rubio E, et al. Bevacizumab in combination with oxaliplatin‐based chemotherapy as first‐line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 2008;26(12):2013‐2019. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
