

Emerging Therapies for COVID-19: The Value of Information From More Clinical Trials
- PMID: 35490085
- PMCID: PMC9045876
- DOI: 10.1016/j.jval.2022.03.016
Emerging Therapies for COVID-19: The Value of Information From More Clinical Trials
Abstract
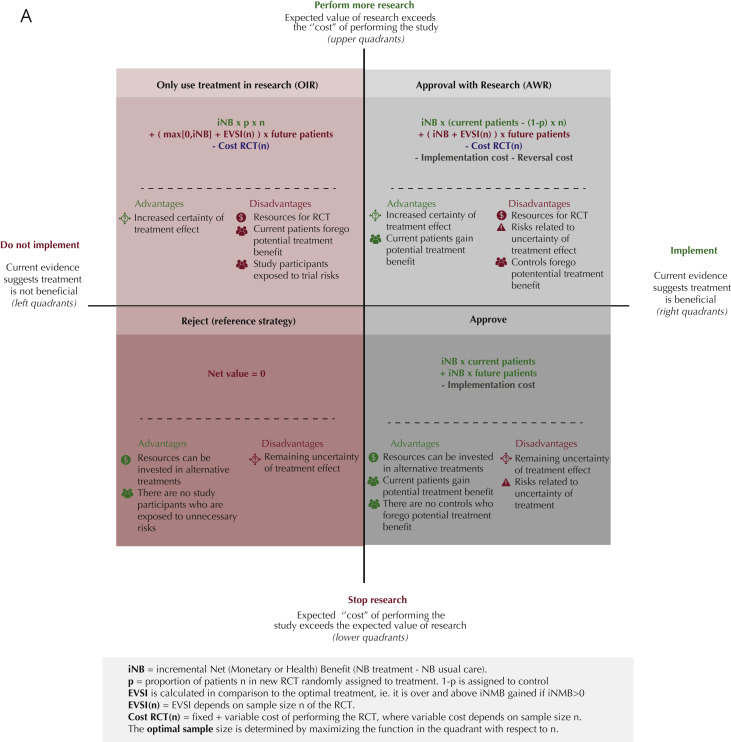
Objectives: The COVID-19 pandemic necessitates time-sensitive policy and implementation decisions regarding new therapies in the face of uncertainty. This study aimed to quantify consequences of approving therapies or pursuing further research: immediate approval, use only in research, approval with research (eg, emergency use authorization), or reject.
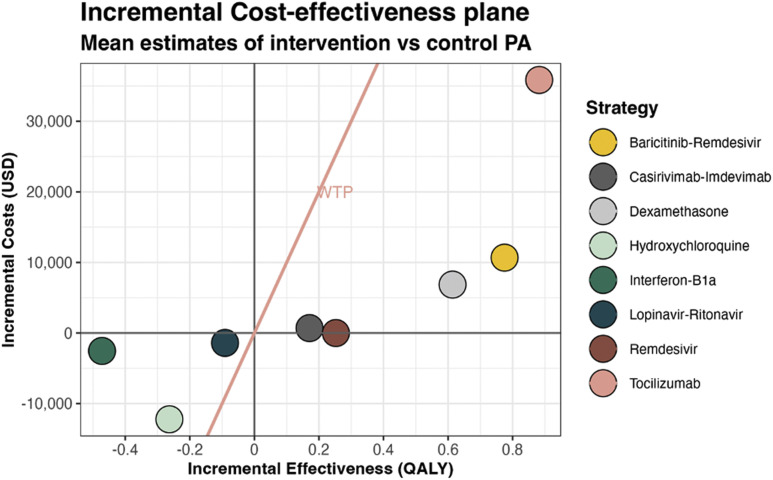
Methods: Using a cohort state-transition model for hospitalized patients with COVID-19, we estimated quality-adjusted life-years (QALYs) and costs associated with the following interventions: hydroxychloroquine, remdesivir, casirivimab-imdevimab, dexamethasone, baricitinib-remdesivir, tocilizumab, lopinavir-ritonavir, interferon beta-1a, and usual care. We used the model outcomes to conduct cost-effectiveness and value of information analyses from a US healthcare perspective and a lifetime horizon.
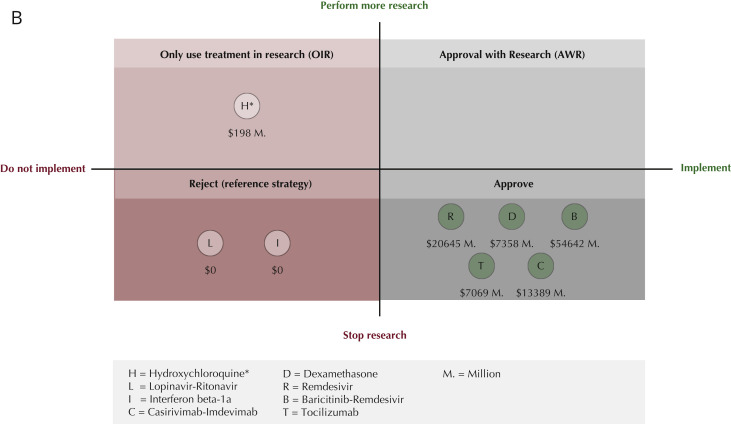
Results: Assuming a $100 000-per-QALY willingness-to-pay threshold, only remdesivir, casirivimab-imdevimab, dexamethasone, baricitinib-remdesivir, and tocilizumab were (cost-) effective (incremental net health benefit 0.252, 0.164, 0.545, 0.668, and 0.524 QALYs and incremental net monetary benefit $25 249, $16 375, $54 526, $66 826, and $52 378). Our value of information analyses suggest that most value can be obtained if these 5 therapies are approved for immediate use rather than requiring additional randomized controlled trials (RCTs) (net value $20.6 billion, $13.4 billion, $7.4 billion, $54.6 billion, and $7.1 billion), hydroxychloroquine (net value $198 million) is only used in further RCTs if seeking to demonstrate decremental cost-effectiveness and otherwise rejected, and interferon beta-1a and lopinavir-ritonavir are rejected (ie, neither approved nor additional RCTs).
Conclusions: Estimating the real-time value of collecting additional evidence during the pandemic can inform policy makers and clinicians about the optimal moment to implement therapies and whether to perform further research.
Keywords: COVID-19; cost-benefit analysis; decision support techniques; drug approval.
Copyright © 2022. Published by Elsevier Inc.
Figures
References
-
- Coronavirus (COVID-19) hospitalizations. Our World in Data. https://ourworldindata.org/covid-hospitalizations
-
- COVID-19 data repository by the Center for Systems Science and Engineering (CSSE) at johns Hopkins University Johns Hopkins University. https://github.com/CSSEGISandData/COVID-19
-
- Van Nguyen T Van, Ferrand G., Cohen-Boulakia S., et al. The COVID-NMA initiative: a living mapping and living systematic review of Covid-19 trials RCT studies on preventive measures and treatments for COVID-19. COVID-NMA consortium. https://covid-nma.com/dataviz/
-
- Claxton K., Palmer S., Longworth L., et al. A comprehensive algorithm for approval of health technologies with, without, or only in research: the key principles for informing coverage decisions. Value Health. 2016;19(6):885–891. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
