

Diminished Immune Surveillance during Histologic Progression of Intraductal Papillary Mucinous Neoplasms Offers a Therapeutic Opportunity for Cancer Interception
- PMID: 35491652
- PMCID: PMC9069801
- DOI: 10.1158/1078-0432.CCR-21-2585
Diminished Immune Surveillance during Histologic Progression of Intraductal Papillary Mucinous Neoplasms Offers a Therapeutic Opportunity for Cancer Interception
Abstract
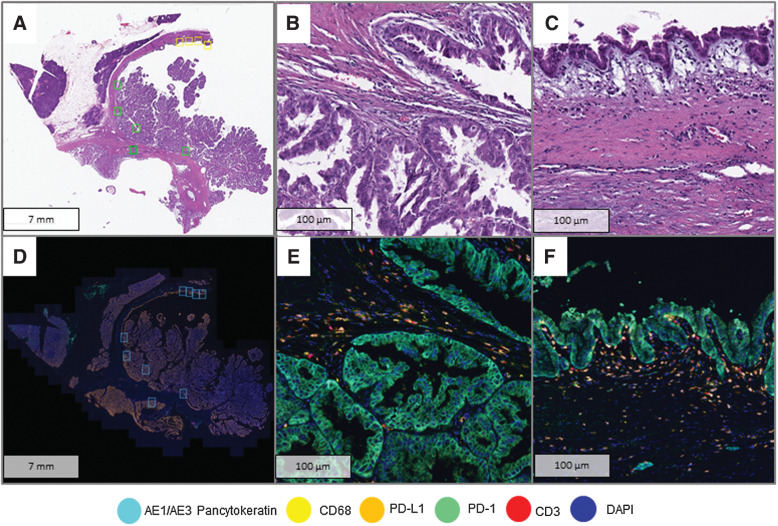
Purpose: Intraductal papillary mucinous neoplasms (IPMN) are bona fide precursors to pancreatic ductal adenocarcinoma (PDAC). While genomic alterations during multistep IPMN progression have been well cataloged, the accompanying changes within the tumor immune microenvironment (TIME) have not been comprehensively studied. Herein, we investigated TIME-related alterations during IPMN progression, using multiplex immunofluorescence (mIF) coupled with high-resolution image analyses.
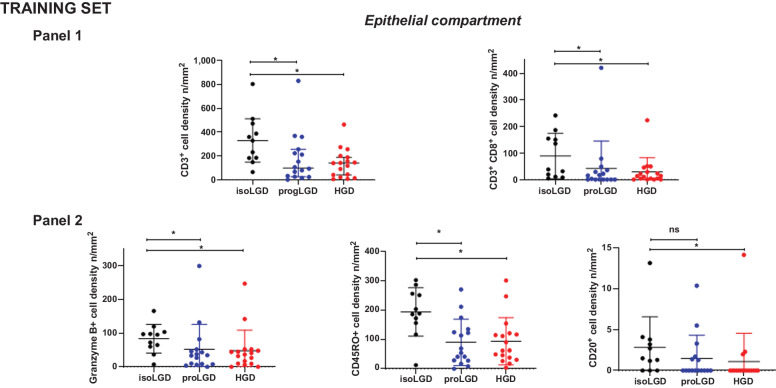
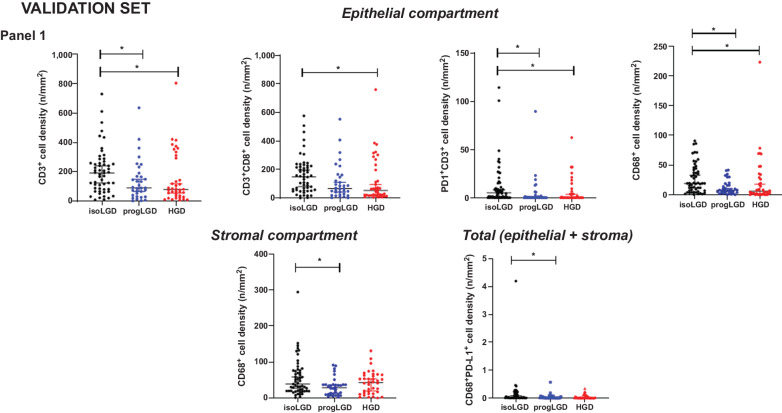
Experimental design: Two sets of formalin-fixed, paraffin-embedded tissue samples from surgically resected IPMNs were analyzed. The training set of 30 samples consisted of 11 low-grade IPMN (LG-IPMN), 17 high-grade IPMN (HG-IPMN), and 2 IPMN with PDAC, while a validation set of 93 samples comprised of 55 LG-IPMN and 38 HG-IPMN. The training set was analyzed with two panels of immuno-oncology-related biomarkers, while the validation set was analyzed with a subset of markers found significantly altered in the training set.
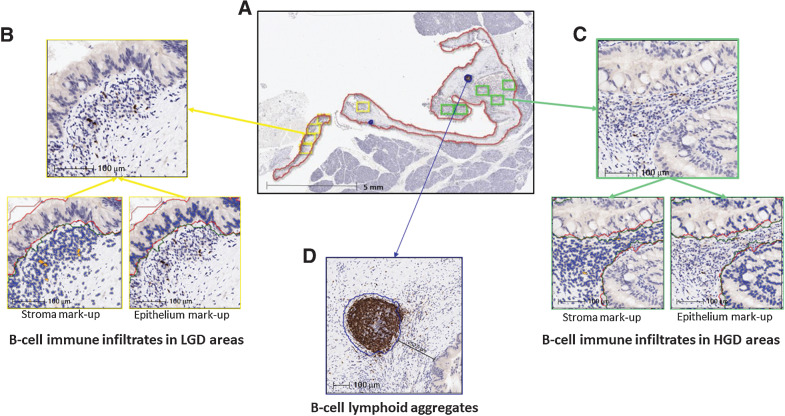
Results: Cell types indicative of enhanced immune surveillance, including cytotoxic and memory T cells, and antigen-experienced T cells and B cells, were all found at higher densities within isolated LG-IPMNs compared with HG-IPMNs. Notably, the TIME of LG-IPMNs that had progressed at the time of surgical resection (progressor LGD) resembled that of the synchronous HG-IPMNs, underscoring that attenuated immune surveillance occurs even in LG-IPMNs destined for progression.
Conclusions: Our findings provide a basis for interception of cystic neoplasia to PDAC, through maintenance of sustained immune surveillance using vaccines and other prevention approaches.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
- Clin Cancer Res. 28:1743.
- Clin Cancer Res. 28:1743.
References
-
- Tanaka M, Fernandez-Del Castillo C, Kamisawa T, Jang JY, Levy P, Ohtsuka T, et al. . Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 2017;17:738–53. - PubMed
-
- Hackert T, Fritz S, Klauss M, Bergmann F, Hinz U, Strobel O, et al. . Main-duct intraductal papillary mucinous neoplasm: high cancer risk in duct diameter of 5 to 9 mm. Ann Surg 2015;262:875–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
