

Medium Cutoff Versus High-Flux Hemodialysis Membranes and Clinical Outcomes: A Cohort Study Using Inverse Probability Treatment Weighting
- PMID: 35492142
- PMCID: PMC9044098
- DOI: 10.1016/j.xkme.2022.100431
Medium Cutoff Versus High-Flux Hemodialysis Membranes and Clinical Outcomes: A Cohort Study Using Inverse Probability Treatment Weighting
Abstract
Rationale & objective: This study investigated the effects on patients' outcomes of using medium cutoff (MCO) versus high-flux (HF) dialysis membranes.
Study design: A retrospective, observational, multicenter, cohort study.
Setting & participants: Patients aged greater than 18 years receiving hemodialysis at the Baxter Renal Care Services dialysis network in Colombia. The inception of the cohort occurred from September 1, 2017, to November 30, 2017, with follow-up to November 30, 2019.
Exposure: The patients were divided into 2 cohorts according to the dialyzer used at the inception: (1) MCO membrane or (2) HF membrane.
Outcomes: Primary outcomes were the hospitalization rate from any cause and hospitalization days per patient-year. Secondary outcomes were acute cardiovascular events and mortality rates from any cause and secondary to cardiovascular causes. Laboratory parameters were assessed throughout the 2-year follow-up period.
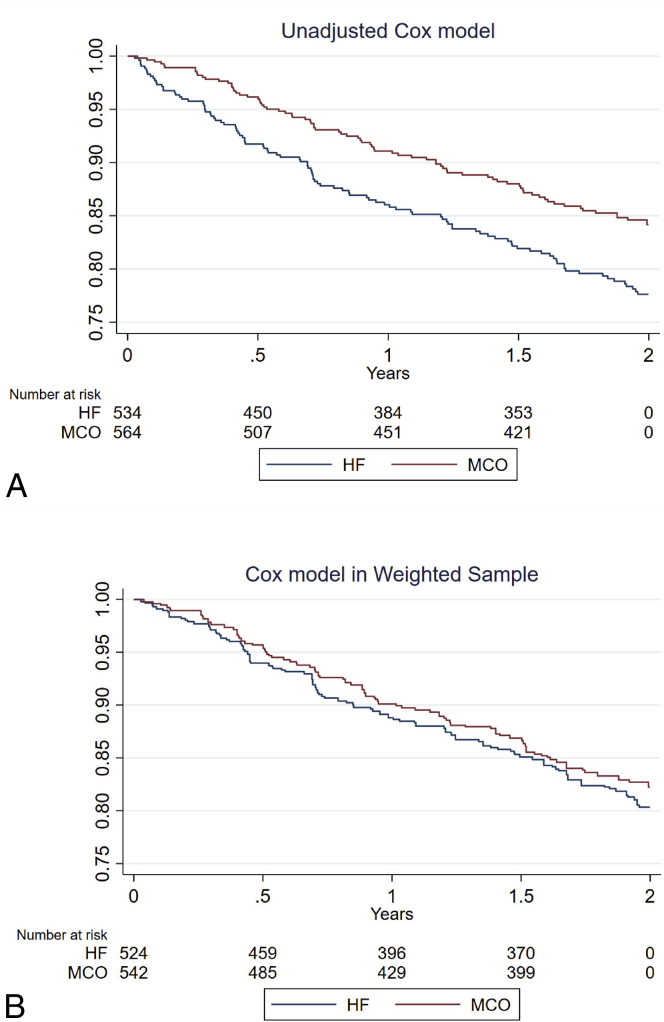
Analytical approach: Descriptive statistics were used to report population characteristics. Inverse probability of treatment weighting was applied to each group before analysis. All categorical variables were compared using Pearson's χ2 test, and continuous variables were analyzed with the t test. Baseline differences between groups with a value of >10% were considered clinically meaningful. Laboratory variables were measured at 5 consecutive time points. A between-patient effect was analyzed using a split-plot factorial analysis of variance.
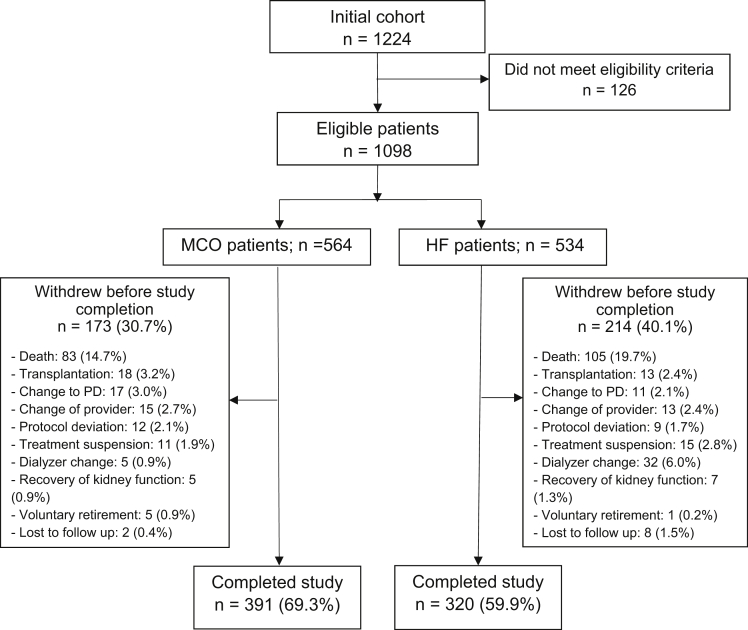
Results: The analysis included 1,098 patients, of whom 564 (51.3%) were dialyzed with MCO membranes and 534 (48.7%) with HF membranes. Patients receiving hemodialysis with MCO membranes had a lower all-cause hospitalization incidence rate (IR) per patient-year (IR = 0.93; 95% CI, 0.82-1.03) than those receiving hemodialysis with HF membranes (IR = 1.13; 95% CI, 0.96-1.30), corresponding to a significant incident rate ratio (MCO/HF) of 0.82 (95% CI, 0.68-0.99; P = 0.04). The frequency of nonfatal cardiovascular events showed statistical significance, with a lower incidence in the MCO group (incident rate ratio = 0.66; 95% CI, 0.46-0.96; P = 0.03). No statistically significant differences in all-cause time until death were observed (P = 0.48). Albumin levels were similar between the 2 dialyzer cohorts.
Limitations: Despite the robust statistical analysis, there remains the possibility that unmeasured variables may still generate residual imbalance and, therefore, skew the results.
Conclusions: The incidences of hospitalization and cardiovascular events in patients receiving hemodialysis were lower when dialyzed with MCO membranes than HF membranes. A randomized controlled trial would be desirable to confirm these results.
Trial registration: Clinical Trials.gov, ISRCTN12403265.
Keywords: Clinical outcomes; dialysis membranes; hemodialysis; high-flux; medium cutoff.
© 2022 The Authors.
Figures


References
-
- Saran R., Bragg-Gresham J.L., Levin N.W., et al. Longer treatment time and slower ultrafiltration in hemodialysis: associations with reduced mortality in the DOPPS. Kidney Int. 2006;69(7):1222–1228. - PubMed
-
- Henderson L.W. Dialysis in the 21st century. Am J Kidney Dis. 1996;28(6):951–957. - PubMed
-
- Oreopoulos D.G. Beyond KT/V: redefining adequacy of dialysis in the 21st century. Int Urol Nephrol. 2002;34(3):393–403. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
