

Association of Cardiometabolic Disease With Cancer in the Community
- PMID: 35492825
- PMCID: PMC9040108
- DOI: 10.1016/j.jaccao.2022.01.095
Association of Cardiometabolic Disease With Cancer in the Community
Abstract
Background: Obesity and cardiometabolic dysfunction have been associated with cancer risk and severity. Underlying mechanisms remain unclear.
Objectives: The aim of this study was to examine associations of obesity and related cardiometabolic traits with incident cancer.
Methods: FHS (Framingham Heart Study) and PREVEND (Prevention of Renal and Vascular End-Stage Disease) study participants without prevalent cancer were studied, examining associations of obesity, body mass index (BMI), waist circumference, visceral adipose tissue (VAT) and subcutaneous adipose tissue depots, and C-reactive protein (CRP) with future cancer in Cox models.
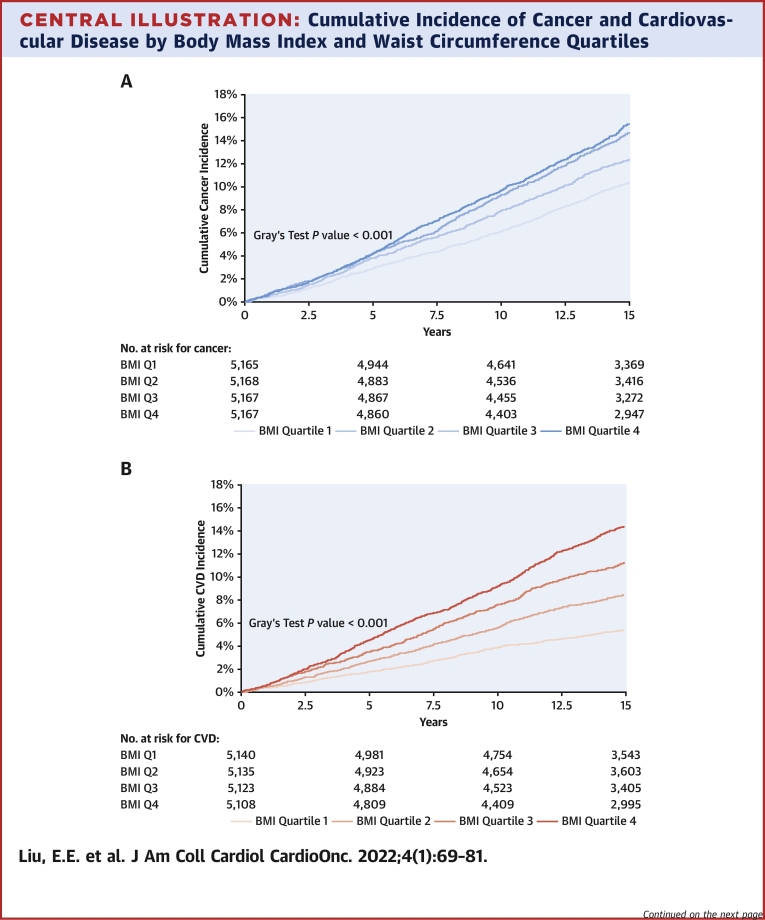
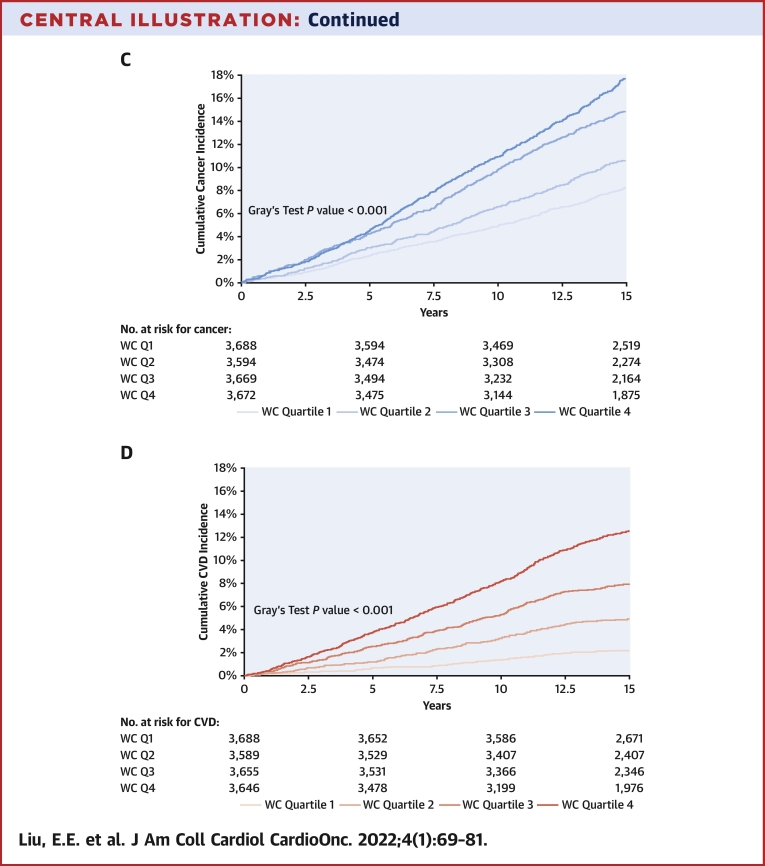
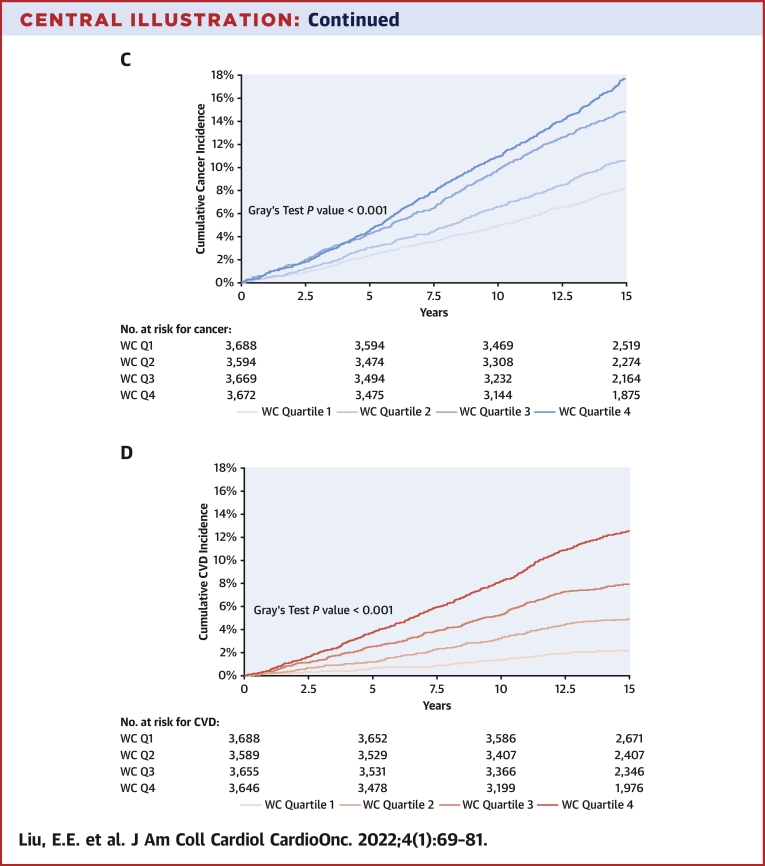
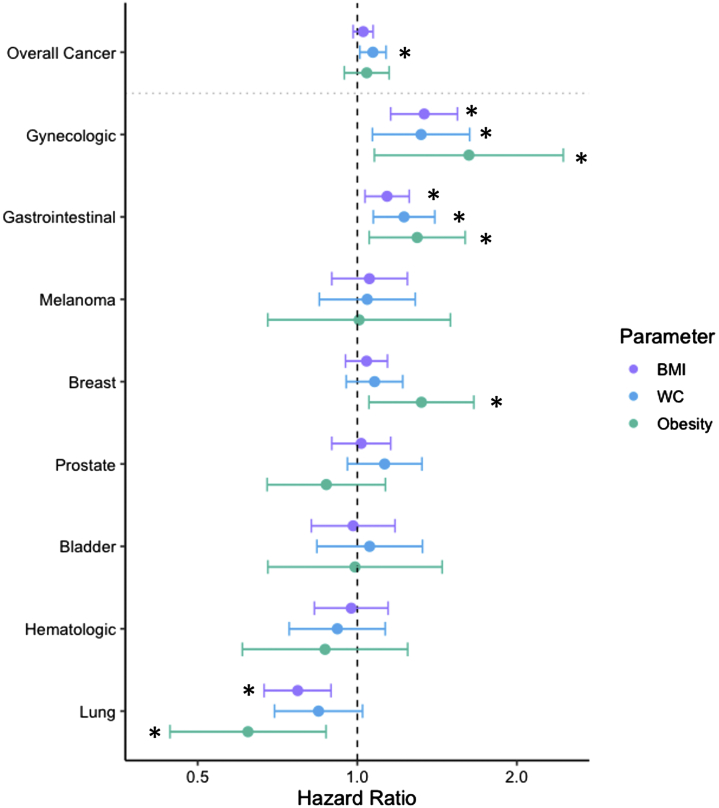
Results: Among 20,667 participants (mean age 50 years, 53% women), 2,619 cancer events were observed over a median follow-up duration of 15 years. Obesity was associated with increased risk for future gastrointestinal (HR: 1.30; 95% CI: 1.05-1.60), gynecologic (HR: 1.62; 95% CI: 1.08-2.45), and breast (HR: 1.32; 95% CI: 1.05-1.66) cancer and lower risk for lung cancer (HR: 0.62; 95% CI: 0.44-0.87). Similarly, waist circumference was associated with increased risk for overall, gastrointestinal, and gynecologic but not lung cancer. VAT but not subcutaneous adipose tissue was associated with risk for overall cancer (HR: 1.22; 95% CI: 1.05-1.43), lung cancer (HR: 1.92; 95% CI: 1.01-3.66), and melanoma (HR: 1.56; 95% CI: 1.02-2.38) independent of BMI. Last, higher CRP levels were associated with higher risk for overall, colorectal, and lung cancer (P < 0.05 for all).
Conclusions: Obesity and abdominal adiposity are associated with future risk for specific cancers (eg, gastrointestinal, gynecologic). Although obesity was associated with lower risk for lung cancer, greater VAT and CRP were associated with higher lung cancer risk after adjusting for BMI.
Keywords: BMI, body mass index; CRP, C-reactive protein; CT, computed tomographic; CVD, cardiovascular disease; HOMA-IR, homeostatic model assessment of insulin resistance; PAI, plasminogen activator inhibitor; SAT, subcutaneous adipose tissue; VAT, visceral adipose tissue; WC, waist circumference; epidemiology; gastrointestinal cancer; inflammation; obesity; risk factor.
© 2022 Published by Elsevier on behalf of the American College of Cardiology Foundation.
Conflict of interest statement
The FHS was supported by contracts from the National Heart, Lung, and Blood Institute (NHLBI) (NO1-HC-25195, HHSN268201500001I, and 75N92019D00031). The PREVEND study was supported by a grant from the Dutch Kidney Foundation (E.033). Dr Ho was supported by grants from the National Institutes of Health (NIH) (R01-HL134893, R01-HL140224, and K24-HL153669). Drs Suthahar and de Boer are supported by grants from the Netherlands Heart Foundation (Netherlands CardioVascular Research Committee [CVON] SHE-PREDICTS-HF, grant 2017-21; CVON RED-CVD, grant 2017-11; CVON PREDICT2, grant 2018-30; and CVON DOUBLE DOSE, grant 2020B005) and by a grant from the European Research Council (Consolidator Grant 818715, SECRETE-HF). Dr Lau was supported by a grant from the NIH (5T32HL094301-07). Dr Cheng has been supported by the NHLBI (grants R01HL131532 and R01HL151828) and Zogenix. Dr Hussain has been supported by the National Cancer Institute (grant R01CA204145). Dr Benjamin was supported by the NIH/NHLBI (grants 2R01 HL092577, 2U54HL120163, and 1R01 HL141434), the NIH/National Institute on Aging (grant 1R01AG066010), the American Heart Association (grant AHA_18SFRN34110082), and the Robert Wood Johnson Foundation (grant 74624). Dr Vasan has been supported in part by the Evans Medical Foundation and the Jay and Louis Coffman Endowment from the Department of Medicine, Boston University School of Medicine. Dr Ho has received research grants from Gilead Sciences and Bayer; and has received research supplies from EcoNugenics. The University Medical Center Groningen, which employs Drs De Boer and Suthahar, has received research grants and/or fees from AstraZeneca, Abbott, Boehringer Ingelheim, Cardior Pharmaceuticals, Ionis Pharmaceuticals, Novo Nordisk, and Roche. Dr de Boer has received speaker fees from Abbott, AstraZeneca, Bayer, Novartis, and Roche. The views expressed in this paper are those of the authors and do not necessarily represent the view of the NHLBI, the NIH, or the U.S. Department of Health and Human Services. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

References
-
- Sung H., Siegel R.L., Torre L.A., et al. Global patterns in excess body weight and the associated cancer burden. CA Cancer J Clin. 2019;69:88–112. - PubMed
-
- Hales C.M., Carroll M.D., Fryar C.D., Ogden C.L. Prevalence of obesity among adults and youth: United States, 2015-2016. NCHS Data Brief No. 288. https://www.cdc.gov/nchs/data/databriefs/db288.pdf Accessed February 9, 2022. - PubMed
-
- Hales C.M., Carroll M.D., Fryar C.D., Ogden C.L. Prevalence of obesity and severe obesity among adults: United States, 2017-2018. NCHS Data Brief No. 360. https://www.cdc.gov/nchs/data/databriefs/db360-h.pdf Accessed February 9, 2022. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
