

Cancer Incidence and Mortality According to Pre-Existing Heart Failure in a Community-Based Cohort
- PMID: 35492831
- PMCID: PMC9040106
- DOI: 10.1016/j.jaccao.2021.11.007
Cancer Incidence and Mortality According to Pre-Existing Heart Failure in a Community-Based Cohort
Abstract
Background: Studies assessing whether heart failure (HF) is associated with cancer and cancer-related mortality have yielded conflicting results.
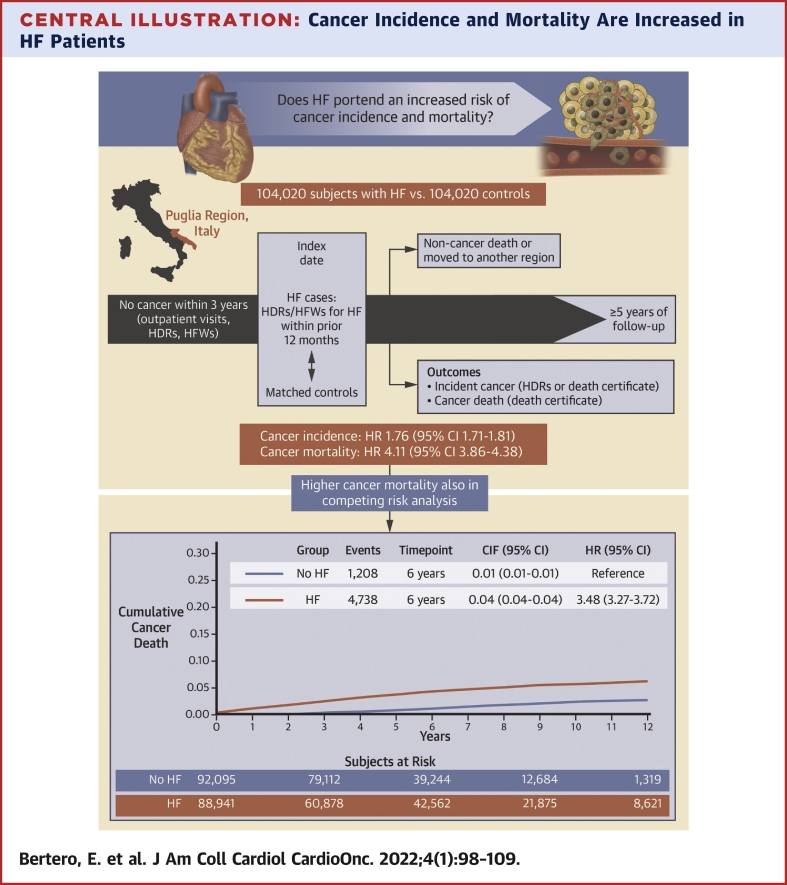
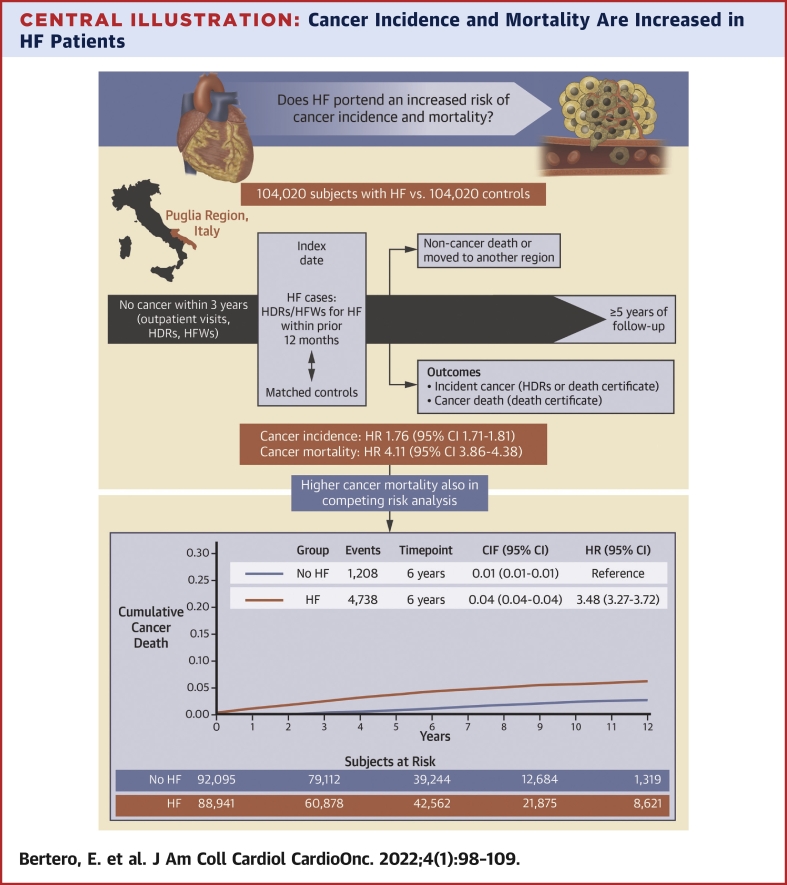
Objectives: This study assessed cancer incidence and mortality according to pre-existing HF in a community-based cohort.
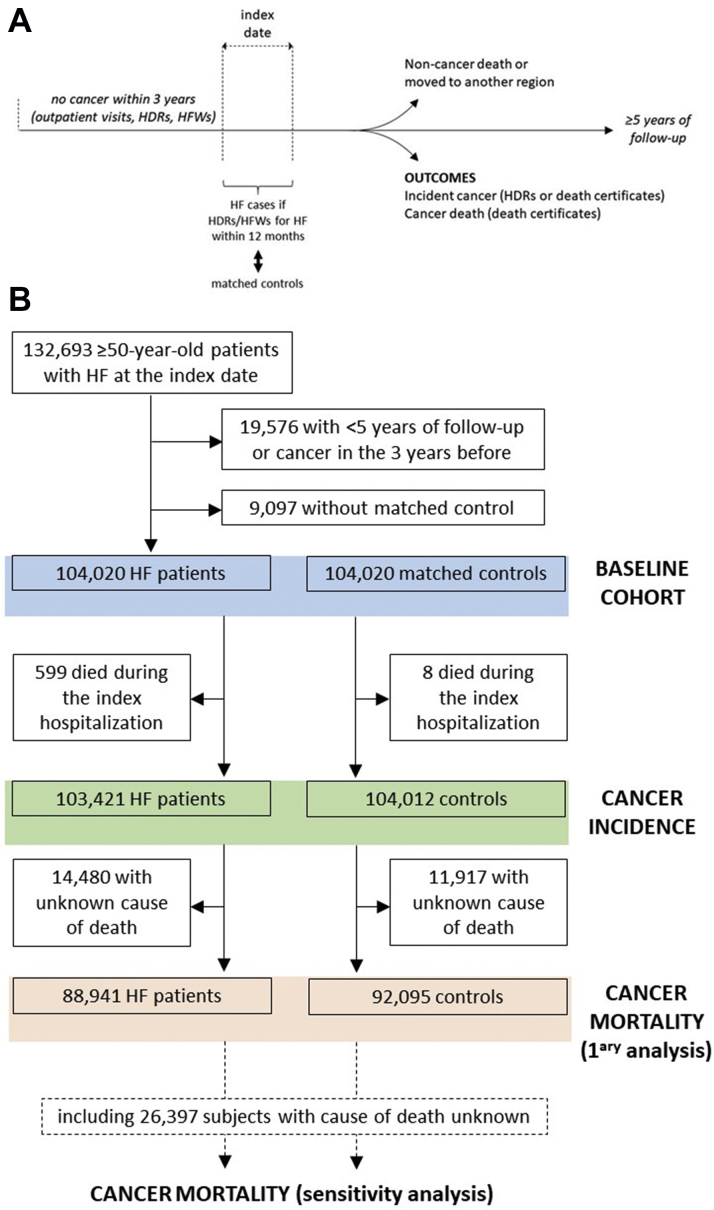
Methods: Among individuals ≥50 years of age from the Puglia region in Italy with administrative health data from 2002 to 2018, no cancer within 3 years before the baseline evaluation, and ≥5-year follow-up, the study matched 104,020 subjects with HF at baseline with 104,020 control subjects according to age, sex, drug-derived complexity index, Charlson comorbidity index, and follow-up duration. Cancer incidence and mortality were defined based on International Classification of Diseases-Ninth Revision codes in hospitalization records or death certificates.
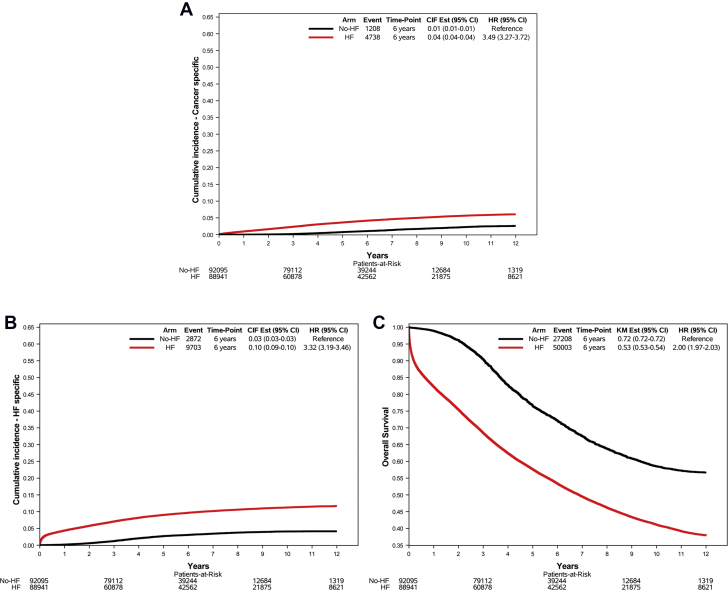
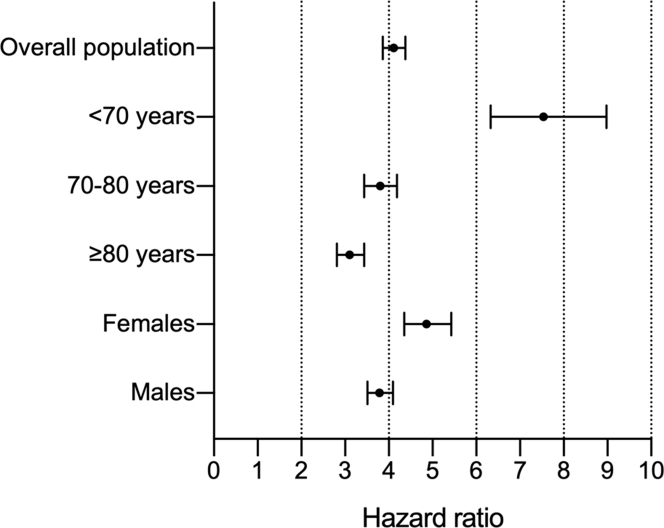
Results: The incidence rate of cancer in HF patients and control subjects was 21.36 (95% CI: 20.98-21.74) and 12.42 (95% CI: 12.14-12.72) per 1000 person-years, respectively, with the HR being 1.76 (95% CI: 1.71-1.81). Cancer mortality was also higher in HF patients than control subjects (HR: 4.11; 95% CI: 3.86-4.38), especially in those <70 years of age (HR: 7.54; 95% CI: 6.33-8.98 vs HR: 3.80; 95% CI: 3.44-4.19 for 70-79 years of age; and HR: 3.10; 95% CI: 2.81-3.43 for ≥80 years of age). The association between HF and cancer mortality was confirmed in a competing risk analysis (subdistribution HR: 3.48; 95% CI: 3.27-3.72). The HF-related excess risk applied to the majority of cancer types. Among HF patients, prescription of high-dose loop diuretic was associated with higher cancer incidence (HR: 1.11; 95% CI: 1.03-1.21) and mortality (HR: 1.35; 95% CI: 1.19-1.53).
Conclusions: HF is associated with an increased risk of cancer and cancer-related mortality, which may be heightened in decompensated states.
Keywords: ATC, Anatomical Therapeutic Chemical; CCI, Charlson comorbidity index; DDCI, drug-derived complexity index; DP, drug prescription; HDR, hospital discharge record; HF, heart failure; HFW, health care cost-related fee waiver; ICD-9-CM, International Classification of Diseases-Ninth Revision-Clinical Modification; IR, incidence rate; SHR, subdistribution HR; cancer; cardio-oncology; comorbidity; heart failure; mortality.
© 2022 The Authors.
Conflict of interest statement
This research was supported by the Italian Ministry of Health (GR-2018-12365661 - CHANGE Study, principal investigator Pietro Ameri) and is part of the work covered by the 2015-2020 Collaboration between the Regional Healthcare Agency of Puglia Region (AReSS Puglia) and the Istituto di Ricerche Farmacologiche Mario Negri IRCCS. Dr Maack was supported by the Barth Syndrome Foundation, the German Research Foundation (Ma 2528/7-1, SFB 894, TRR-219), and the German Federal Agency for Education and Research (01EO1504). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Ameri P., Canepa M., Anker M.S., et al. Cancer diagnosis in patients with heart failure: epidemiology, clinical implications and gaps in knowledge. Eur J Heart Fail. 2018;20:879–887. - PubMed
-
- Bertero E., Canepa M., Maack C., Ameri P. Linking heart failure to cancer. Circulation. 2018;138:735–742. - PubMed
-
- Duarte C.W., Lindner V., Francis S.A., Schoormans D. Visualization of cancer and cardiovascular disease co-occurrence with network methods. JCO Clin Cancer Inform. 2017;1:1–12. - PubMed
-
- Chao C., Xu L., Bhatia S., et al. Cardiovascular disease risk profiles in survivors of adolescent and young adult (AYA) cancer: the Kaiser Permanente AYA Cancer Survivors Study. J Clin Oncol. 2016;34:1626–1633. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
