

Peptides-Coated Oncolytic Vaccines for Cancer Personalized Medicine
- PMID: 35493448
- PMCID: PMC9047942
- DOI: 10.3389/fimmu.2022.826164
Peptides-Coated Oncolytic Vaccines for Cancer Personalized Medicine
Abstract
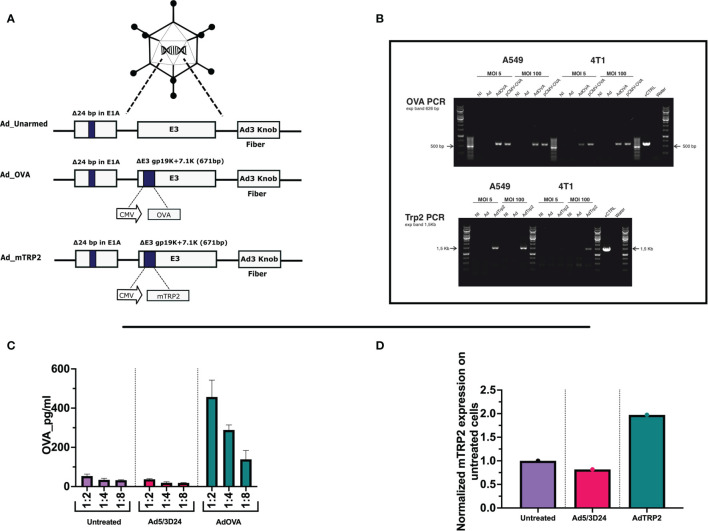
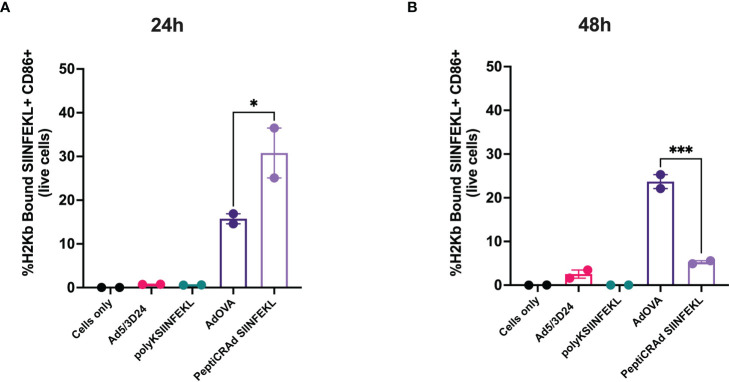
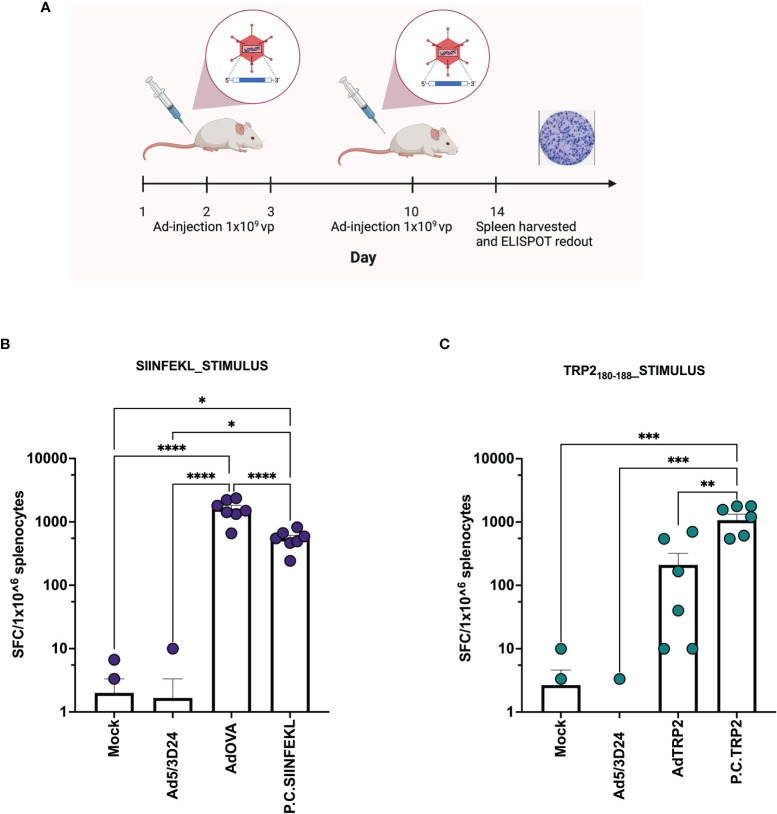
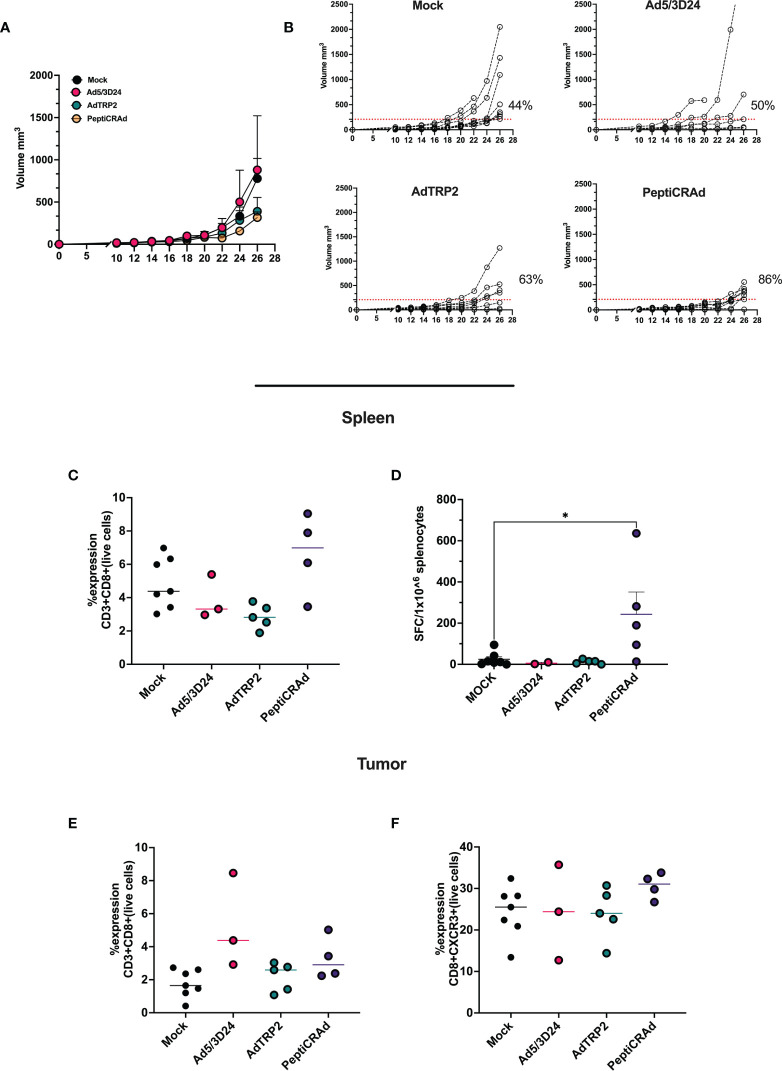
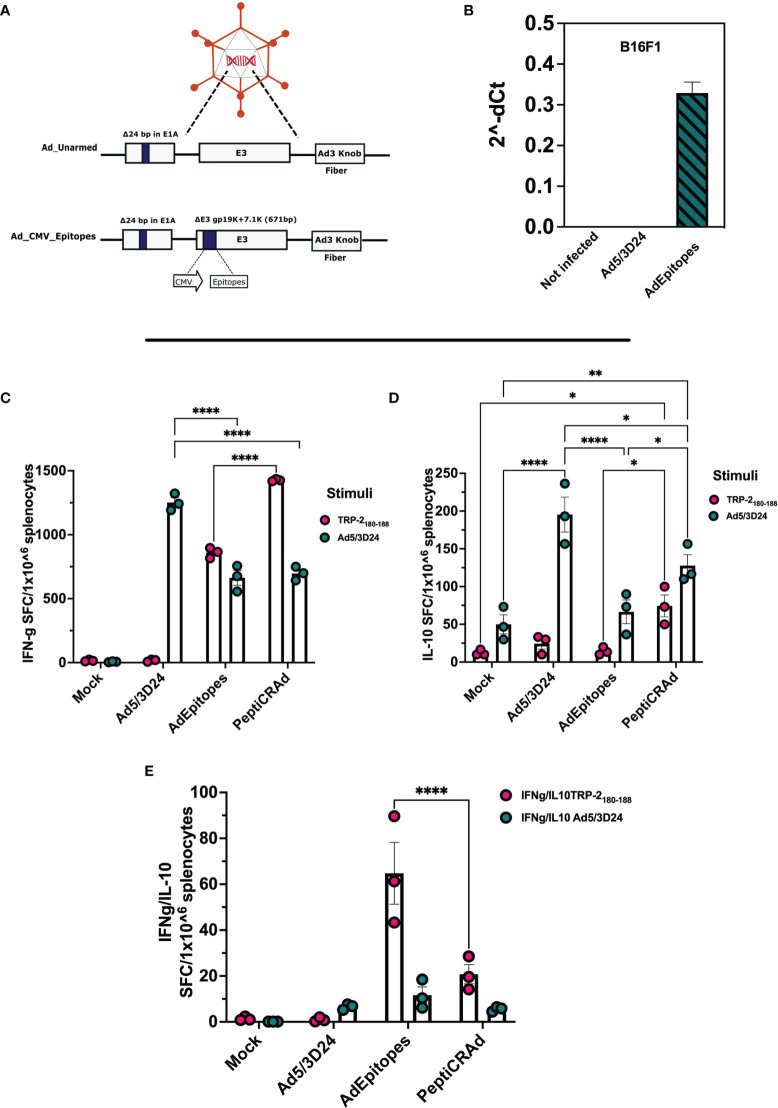
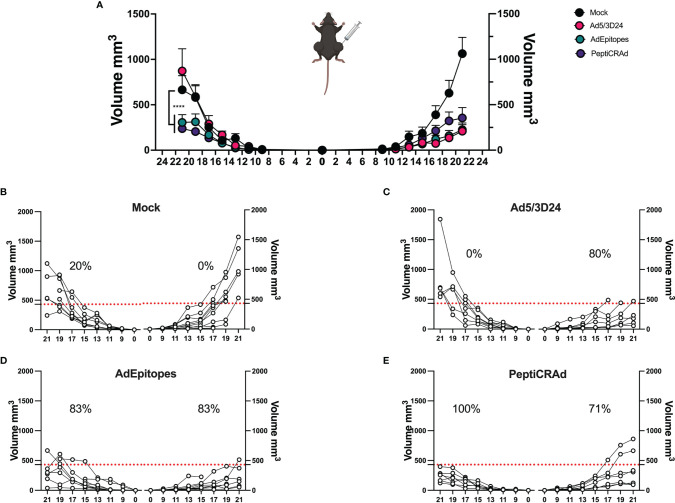
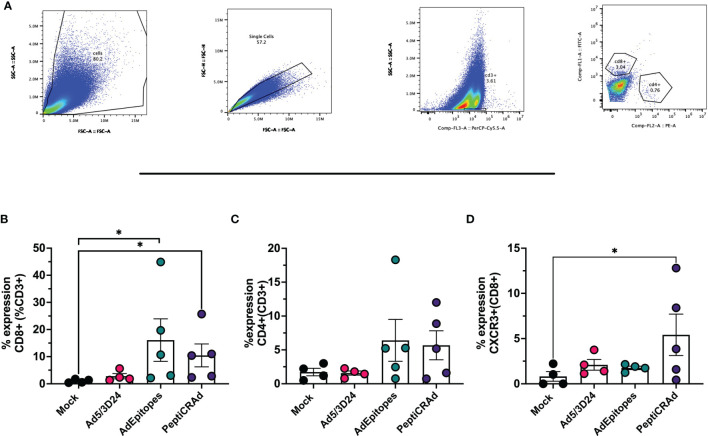
Oncolytic Viruses (OVs) work through two main mechanisms of action: the direct lysis of the virus-infected cancer cells and the release of tumor antigens as a result of the viral burst. In this sc.enario, the OVs act as in situ cancer vaccines, since the immunogenicity of the virus is combined with tumor antigens, that direct the specificity of the anti-tumor adaptive immune response. However, this mechanism in some cases fails in eliciting a strong specific T cell response. One way to overcome this problem and enhance the priming efficiency is the production of genetically modified oncolytic viruses encoding one or more tumor antigens. To avoid the long and expensive process related to the engineering of the OVs, we have exploited an approach based on coating OVs (adenovirus and vaccinia virus) with tumor antigens. In this work, oncolytic viruses encoding tumor antigens and tumor antigen decorated adenoviral platform (PeptiCRAd) have been used as cancer vaccines and evaluated both for their prophylactic and therapeutic efficacy. We have first tested the oncolytic vaccines by exploiting the OVA model, moving then to TRP2, a more clinically relevant tumor antigen. Finally, both approaches have been investigated in tumor neo-antigens settings. Interestingly, both genetically modified oncolytic adenovirus and PeptiCRAd elicited T cells-specific anti-tumor responses. However, in vitro cross-representation experiments, showed an advantage of PeptiCRAd as regards the fast presentation of the model epitope SIINFEKL from OVA in an immunogenic rather than tolerogenic fashion. Here two approaches used as cancer oncolytic vaccines have been explored and characterized for their efficacy. Although the generation of specific anti-tumor T cells was elicited in both approaches, PeptiCRAd retains the advantage of being rapidly adaptable by coating the adenovirus with a different set of tumor antigens, which is crucial in personalized cancer vaccines clinical setting.
Keywords: PeptiCRAd; cancer vaccines; oncolytic viruses; personalized medicine; tumor antigens.
Copyright © 2022 Feola, Russo, Martins, Lopes, Vandermeulen, Fluhler, De Giorgi, Fusciello, Pesonen, Ylösmäki, Antignani, Chiaro, Hamdan, Feodoroff, Grönholm and Cerullo.
Conflict of interest statement
VC is a co-founder and shareholder at VALO Therapeutics. SP is an employee and a shareholder at VALO Therapeutics. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Rabu C, Rangan L, Florenceau L, Fortun A, Charpentier M, Dupre E, et al. . Cancer Vaccines: Designing Artificial Synthetic Long Peptides to Improve Presentation of Class I and Class II T Cell Epitopes by Dendritic Cells. Oncoimmunology (2019) 8(4):e1560919. doi: 10.1080/2162402X.2018.1560919 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical