

Potential Impact of Rapid Multiplex PCR on Antimicrobial Therapy Guidance for Ventilated Hospital-Acquired Pneumonia in Critically Ill Patients, A Prospective Observational Clinical and Economic Study
- PMID: 35493730
- PMCID: PMC9043525
- DOI: 10.3389/fcimb.2022.804611
Potential Impact of Rapid Multiplex PCR on Antimicrobial Therapy Guidance for Ventilated Hospital-Acquired Pneumonia in Critically Ill Patients, A Prospective Observational Clinical and Economic Study
Abstract
Objectives: To investigate the potential impact of the syndromic multiplex FilmArray® Pneumonia plus Panel (FAPP) on the antimicrobial treatment guidance of patients with ventilated hospital-acquired pneumonia (VHAP).
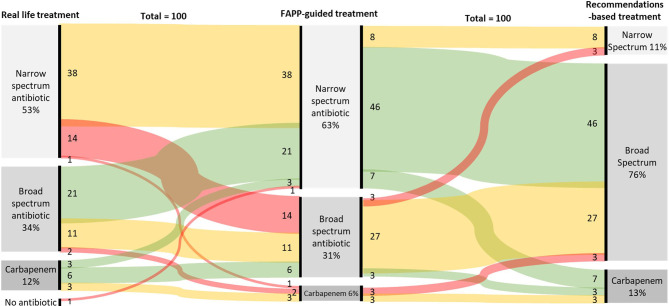
Methods: Respiratory fluids from 100 adult patients with VHAP, receiving invasive mechanical ventilation in three intensive care units from one French university hospital, were tested prospectively using FAPP. Conventional cultures were performed in parallel as routine practice. Clinicians were left blinded to the FAPP results. Antimicrobial therapies based on FAPP results were simulated by independent blinded experts according to a predefined algorithm and compared to 1) those prescribed in practice according to local guidelines (real-life), and 2) those that complied with the international ERS/ESICM/ESCMID/ALAT recommendations. The primary endpoint was the number of days of broad-spectrum antimicrobial therapy. Secondary endpoints were the rates of microbiological treatment failure and cost-effectiveness ratio.
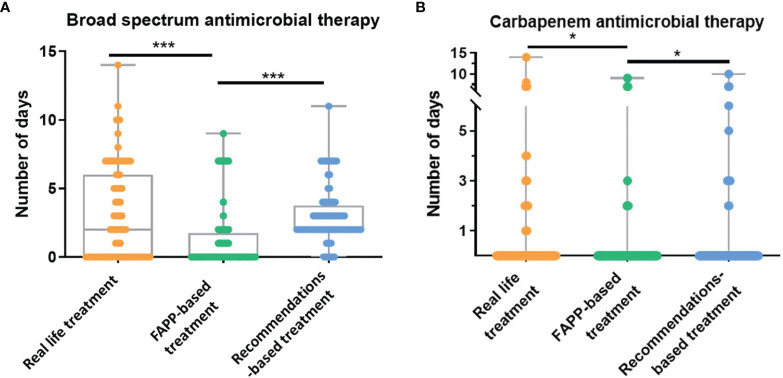
Results: The predicted median duration of broad-spectrum antibiotics was 0 [0-1.25] day in the FAPP-based simulation, versus 2 [0-6] days in real-life (p<0.0001) and 2 [2-3.25] days in the recommendations-based simulation (p<0.0001). Treatment failure was predicted in 3% of cases with FAPP results versus observed in 11% in real-life (p=0.08) and 6% with recommendations-based simulation (p=0.37). The incremental cost-effectiveness ratio was 1 121 € [-7021; 6794] to avoid one day of non-optimized antimicrobial therapy.
Conclusions: Our results suggest that using FAPP in patients with VHAP has the potential to reduce the use of broad-spectrum antimicrobial therapy without increasing the risk of microbial treatment failure.
Keywords: biomolecular diagnosis; empiric treatment; hospital-acquired pneumonia; intensive care unit; pneumonia.
Copyright © 2022 Guillotin, Poulain, Gaborit, Bouras, Cinotti, Lakhal, Vourc’h, Rozec, Asehnoune, Vibet, Riche, Gibaud, Crémet and Roquilly.
Conflict of interest statement
Author BG was employed by Service de Maladies Infectieuses et Tropicales et CIC 1413. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Braykov N. P., Morgan D. J., Schweizer M. L., Uslan D. Z., Kelesidis T., Weisenberg S. A., et al. . (2014). Assessment of Empirical Antibiotic Therapy Optimisation in Six Hospitals: An Observational Cohort Study. Lancet Infect. Dis. 14, 1220–1227. doi: 10.1016/S1473-3099(14)70952-1 - DOI - PMC - PubMed
-
- Buchan B. W., Windham S., Balada-Llasat J. -M., Leber A., Harrington A., Relich R., et al. . (2020). Practical Comparison of the Biofire® Filmarray® Pneumonia Panel to Routine Diagnostic Methods and Potential Impact on Antimicrobial Stewardship in Adult Hospitalized Patients With Lower Respiratory Tract Infections. J. Clin. Microbiol. 58 (7). doi: 10.1128/JCM.00135-20 - DOI - PMC - PubMed
-
- Cambau E., Durand-Zaleski I., Bretagne S., Brun-Buisson C., Cordonnier C., Duval X., et al. . (2017). Performance and Economic Evaluation of the Molecular Detection of Pathogens for Patients With Severe Infections: The EVAMICA Open-Label, Cluster-Randomised, Interventional Crossover Trial. Intensive Care Med. 43, 1613–1625. doi: 10.1007/s00134-017-4766-4 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources