

Non-Invasive Neuromodulation in the Rehabilitation of Pisa Syndrome in Parkinson's Disease: A Randomized Controlled Trial
- PMID: 35493824
- PMCID: PMC9046718
- DOI: 10.3389/fneur.2022.849820
Non-Invasive Neuromodulation in the Rehabilitation of Pisa Syndrome in Parkinson's Disease: A Randomized Controlled Trial
Abstract
Background: Pisa syndrome (PS) is a frequent postural complication of Parkinson's disease (PD). PS poorly responds to anti-parkinsonian drugs and the improvement achieved with neurorehabilitation tends to fade in 6 months or less. Transcranial direct current stimulation (t-DCS) is a non-invasive neuromodulation technique that showed promising results in improving specific symptoms in different movement disorders.
Objectives: This study aimed to evaluate the role of bi-hemispheric t-DCS as an add-on to a standardized hospital rehabilitation program in the management of PS in PD.
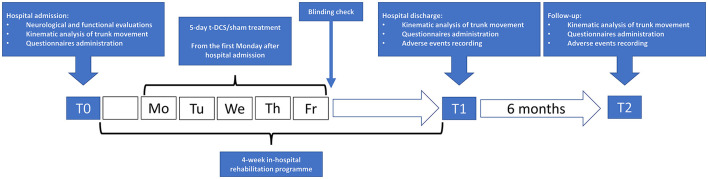
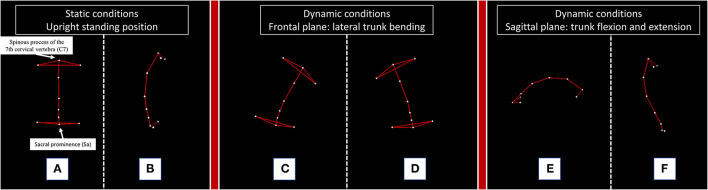
Methods: This study included 28 patients with PD and PS (21 men, aged 72.9 ± 5.1 years) who underwent a 4-week intensive neurorehabilitation treatment and were randomized to receive: i) t-DCS (t-DCS group, n = 13) for 5 daily sessions (20 min-2 mA) with bi-hemispheric stimulation over the primary motor cortex (M1), or ii) sham stimulation (sham group, n = 15) with the same duration and cadence. At baseline (T0), end of rehabilitation (T1), and 6 months later (T2) patients were evaluated with both trunk kinematic analysis and clinical scales, including UPDRS-III, Functional Independence Measure (FIM), and Numerical Rating Scale for lumbar pain.
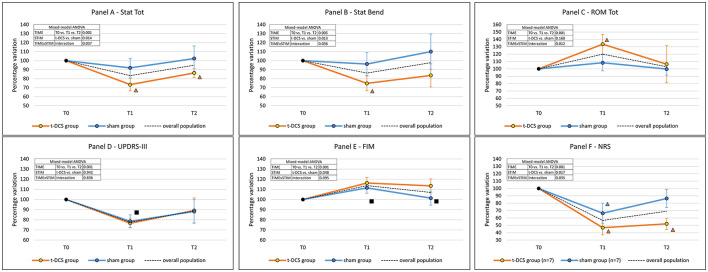
Results: When compared to the sham group, the t-DCS group achieved a more pronounced improvement in several variables: overall posture (p = 0.014), lateral trunk inclination (p = 0.013) during upright standing position, total range of motion of the trunk (p = 0.012), FIM score (p = 0.048), and lumbar pain intensity (p = 0.017).
Conclusions: Our data support the use of neuromodulation with t-DCS as an add-on to neurorehabilitation for the treatment of patients affected by PS in PD.
Keywords: lateral trunk inclination; movement analysis; movement disorders; neurorehabilitation; parkinsonism; transcranial direct current stimulation (tDCS).
Copyright © 2022 De Icco, Putortì, Allena, Avenali, Dagna, Martinelli, Cristina, Grillo, Fresia, Bitetto, Cosentino, Valentino, Alfonsi, Sandrini, Pisani and Tassorelli.
Conflict of interest statement
RD, APu, MAl, MAv, CD, DM, SC, VG, MF, VB, GC, FV, GS, and EA report no funding in the preceding 12 months. APi holds grants that are not related to the subject of the present study, and he reports no biomedical financial interests or potential conflicts of interest. CT received honoraria for their participation in advisory boards or for oral presentations from Allergan, ElectroCore, Eli-Lilly, Novartis, and Teva. CT has no ownership interest and does not own stocks of any pharmaceutical company. CT serves as Chief Section Editor of Frontiers in Neurology—Section Headache Medicine and Facial Pain and on the editorial board of The Journal of Headache and Pain.
Figures
References
-
- Tassorelli C, De Icco R, Alfonsi E, Bartolo M, Serrao M, Avenali M, et al. . Botulinum toxin type A potentiates the effect of neuromotor rehabilitation of Pisa syndrome in Parkinson disease: a placebo controlled study. Park Relat Disord. (2014) 20:1140–4. 10.1016/j.parkreldis.2014.07.015 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous