

Radioisotope-Guided Sentinel Lymph Node Biopsy in Penile Cancer: A Long-Term Follow-Up Study
- PMID: 35494039
- PMCID: PMC9046689
- DOI: 10.3389/fonc.2022.850905
Radioisotope-Guided Sentinel Lymph Node Biopsy in Penile Cancer: A Long-Term Follow-Up Study
Abstract
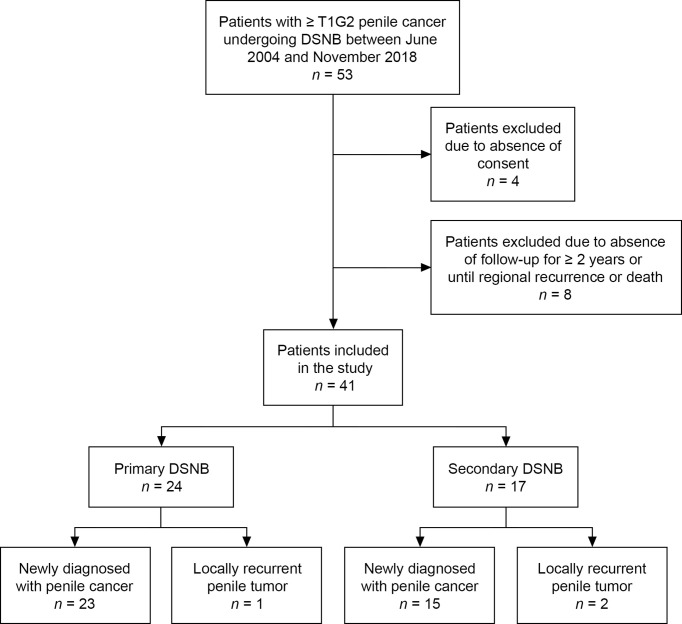
Lymph node (LN) management is critical for survival in patients with penile cancer. However, radical inguinal lymphadenectomy carries a high risk of postoperative complications such as lymphedema, lymphocele, wound infection, and skin necrosis. The European Association of Urology guidelines therefore recommend invasive LN staging by modified inguinal lymphadenectomy or dynamic sentinel node biopsy (DSNB) in clinically node-negative patients (cN0) with intermediate- and high-risk tumors (≥ T1G2). However, the timing of DSNB (simultaneous vs. subsequent to partial or total penile resection) is controversial and the low incidence of penile cancer means that data on the long-term outcomes of DSNB are limited. The present study aimed to analyze the reliability and morbidity of DSNB in patients with penile cancer during long-term follow-up. This retrospective study included 41 patients (76 groins) who underwent radioisotope-guided DSNB simultaneously or secondarily after penile surgery from June 2004 to November 2018. In total, 193 sentinel LNs (SLNs) and 39 non-SLNs were removed. The median number of dissected LNs was 2.5 (interquartile range 2-4). Histopathological analysis showed that five of the 76 groins (6.6%) contained metastases. None of the non-SLNs were tumor-positive. In accordance with the guidelines, all inguinal regions with positive SLNs underwent secondary radical inguinal lymphadenectomy, which revealed three additional metastases in one groin. Regional LN recurrence was detected in three patients (four groins) during a median follow-up of 70 months, including two patients in whom DSNB had been performed secondarily after repetitive penile tumor resections. DSNB-related complications occurred in 15.8% of groins. Most complications were mild (Clavien-Dindo grade I; 50%) or moderate (II; 25%), and invasive intervention was only required in 3.9% of groins (IIIa: n = 1; IIIb: n = 2). In summary, this study suggests that the current radioisotope-guided DSNB procedure may reduce the complication rate of inguinal lymphadenectomy in patients with cN0 penile cancer. However, DSNB and penile surgery should be performed simultaneously to minimize the false-negative rate. Recent advances, such as new tracers and imaging techniques, may help to reduce the false-negative rate of DSNB further.
Keywords: dynamic sentinel node biopsy; inguinal lymphadenectomy; lymph node metastases; penile cancer; sentinel lymph node.
Copyright © 2022 Nemitz, Vincke, Michalik, Engels, Meyer, Henke, Wawroschek and Winter.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Reliability of radioisotope-guided sentinel lymph node biopsy in penile cancer: verification in consideration of the European guidelines.BMC Urol. 2015 Sep 28;15:98. doi: 10.1186/s12894-015-0093-7. BMC Urol. 2015. PMID: 26416391 Free PMC article.
-
Reliability of dynamic sentinel node biopsy combined with ultrasound-guided removal of sonographically suspicious lymph nodes as a diagnostic approach in patients with penile cancer with palpable inguinal lymph nodes.Urol Oncol. 2015 Sep;33(9):389.e9-14. doi: 10.1016/j.urolonc.2015.03.022. Epub 2015 Apr 29. Urol Oncol. 2015. PMID: 25934562
-
Feasibility of performing dynamic sentinel lymph node biopsy as a delayed procedure in penile cancer.World J Urol. 2016 Mar;34(3):329-35. doi: 10.1007/s00345-015-1577-5. Epub 2015 Jun 10. World J Urol. 2016. PMID: 26060137
-
Management of the lymph nodes in penile cancer.Urology. 2010 Aug;76(2 Suppl 1):S43-57. doi: 10.1016/j.urology.2010.03.001. Urology. 2010. PMID: 20691885 Review.
-
Minimally invasive evaluation of the clinically negative inguinal node in penile cancer: Dynamic sentinel node biopsy.Urol Oncol. 2022 Jun;40(6):209-214. doi: 10.1016/j.urolonc.2020.11.012. Epub 2020 Nov 18. Urol Oncol. 2022. PMID: 33218920 Review.
Cited by
-
New EAU/ASCO guideline recommendations on sentinel node biopsy for penile cancer and remaining challenges from a nuclear medicine perspective.Eur J Nucl Med Mol Imaging. 2024 Aug;51(10):2861-2868. doi: 10.1007/s00259-023-06586-6. Epub 2024 Jan 13. Eur J Nucl Med Mol Imaging. 2024. PMID: 38216778
References
LinkOut - more resources
Full Text Sources