

The Effects of Menopause Hormone Therapy on Lipid Profile in Postmenopausal Women: A Systematic Review and Meta-Analysis
- PMID: 35496275
- PMCID: PMC9039020
- DOI: 10.3389/fphar.2022.850815
The Effects of Menopause Hormone Therapy on Lipid Profile in Postmenopausal Women: A Systematic Review and Meta-Analysis
Abstract
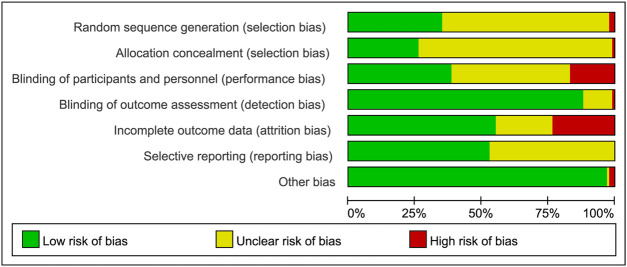
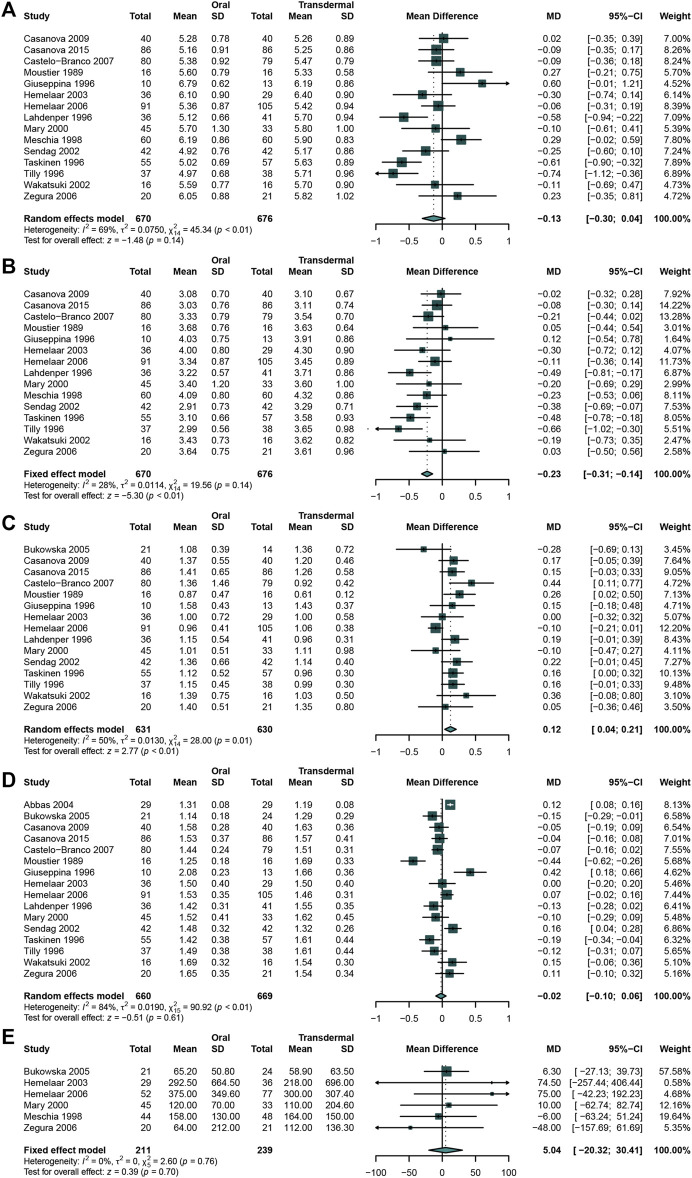
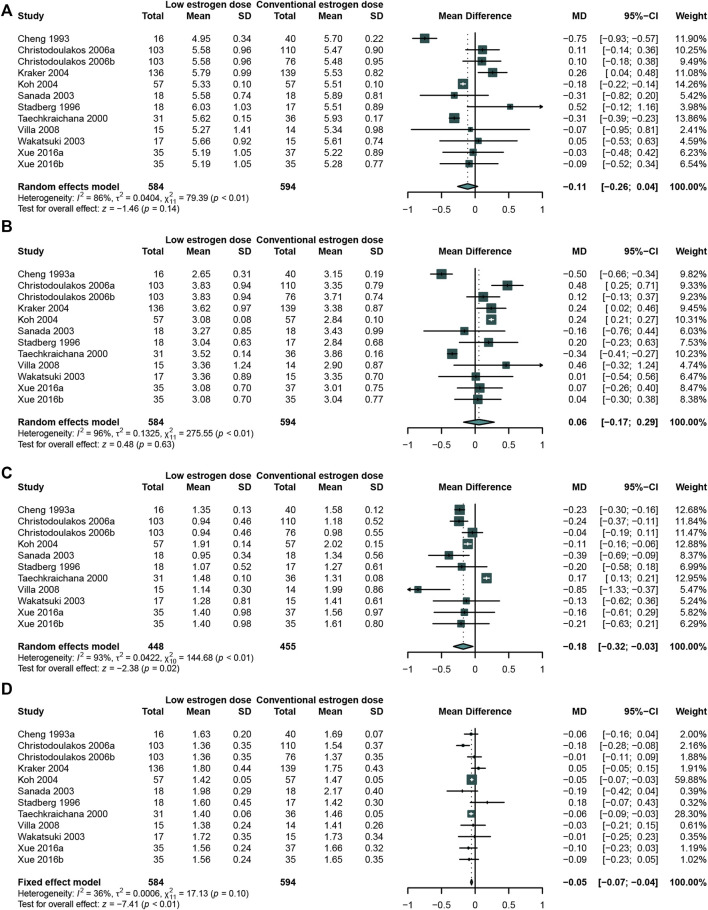
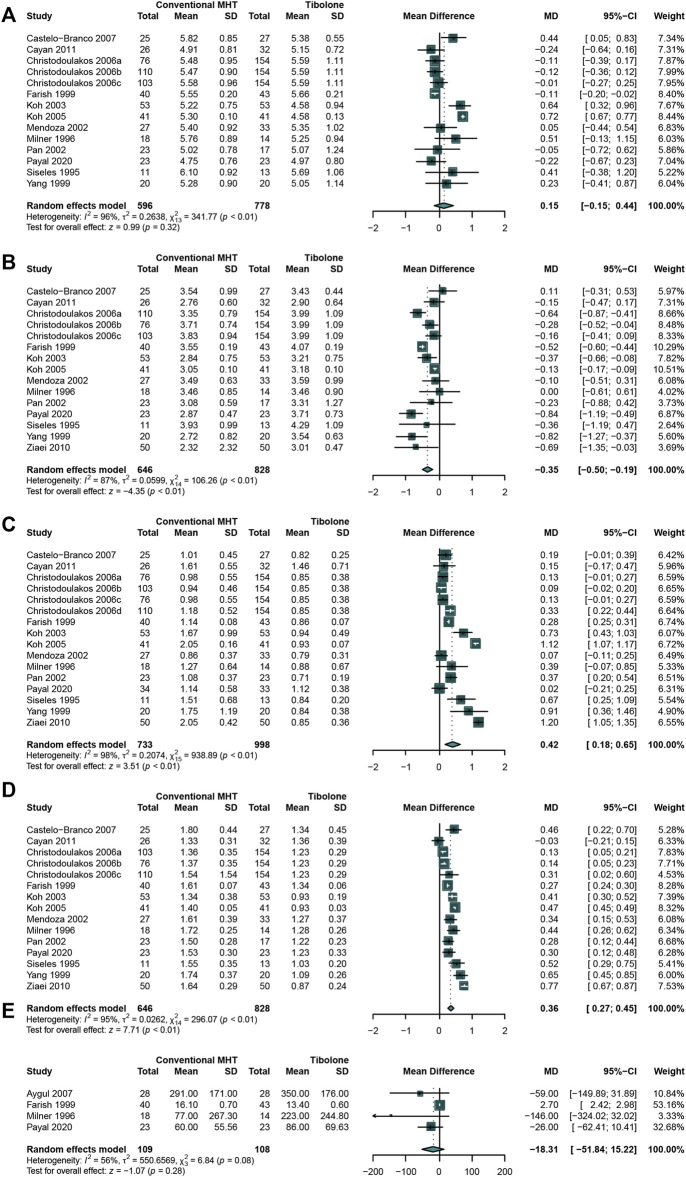
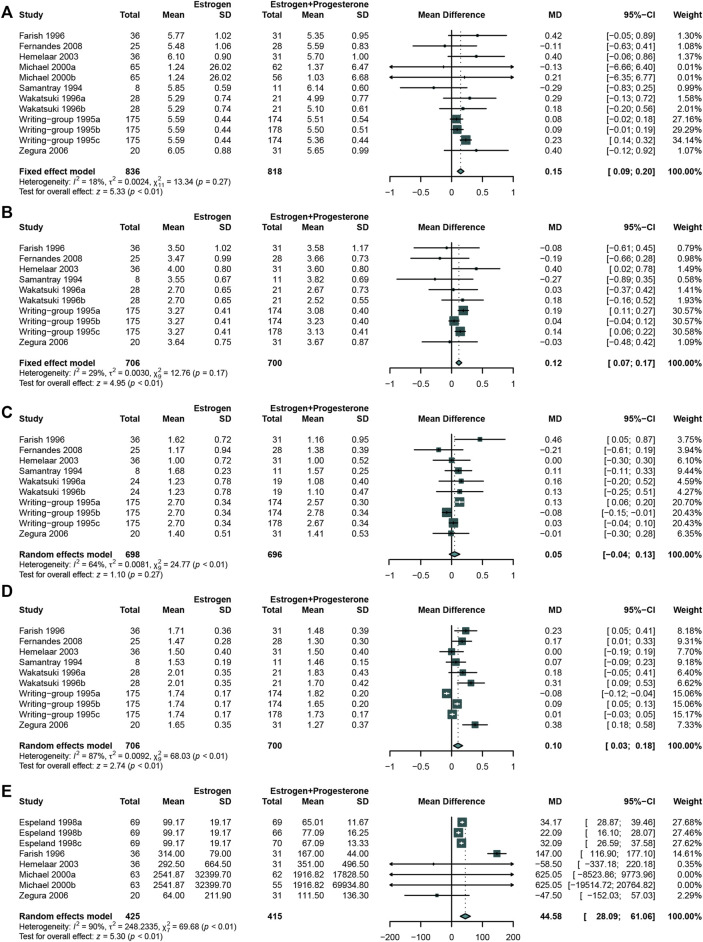
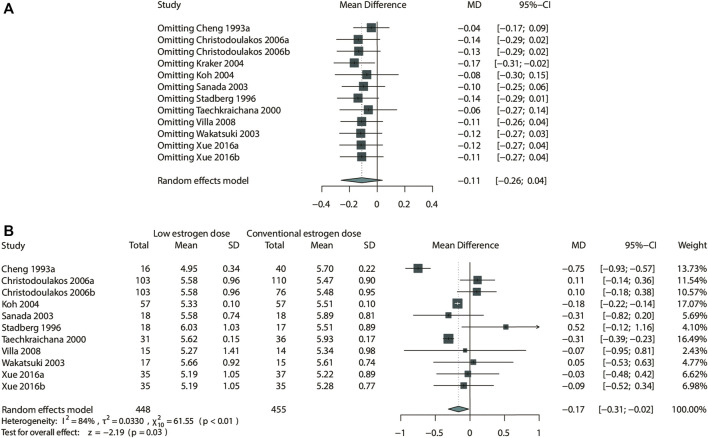
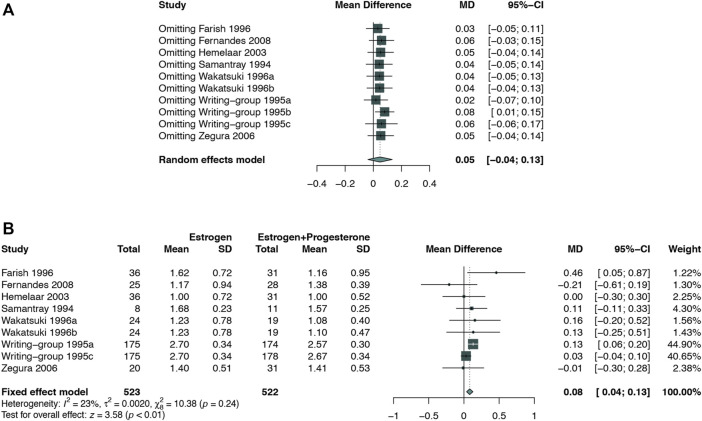
Importance: The incidence of dyslipidemia increases after menopause. Menopause hormone therapy (MHT) is recommended for menopause related disease. However, it is benefit for lipid profiles is inconclusive. Objective: To conduct a systematic review and meta-analysis of randomized controlled trials to evaluate the effects of MHT on lipid profile in postmenopausal women. Evidence Review: Related articles were searched on PubMed/Medline, EMBASE, Web of Science, and Cochrane Library databases from inception to December 2020. Data extraction and quality evaluation were performed independently by two reviewers. The methodological quality was assessed using the "Cochrane Risk of Bias checklist". Results: Seventy-three eligible studies were selected. The results showed that MHT significantly decreased the levels of TC (WMD: -0.43, 95% CI: -0.53 to -0.33), LDL-C (WMD: -0.47, 95% CI: -0.55 to -0.40) and LP (a) (WMD: -49.46, 95% CI: -64.27 to -34.64) compared with placebo or no treatment. Oral MHT led to a significantly higher TG compared with transdermal MHT (WMD: 0.12, 95% CI: 0.04-0.21). The benefits of low dose MHT on TG was also concluded when comparing with conventional-dose estrogen (WMD: -0.18, 95% CI: -0.32 to -0.03). The results also showed that conventional MHT significantly decreased LDL-C (WMD: -0.35, 95% CI: -0.50 to -0.19), but increase TG (WMD: 0.42, 95%CI: 0.18-0.65) compared with tibolone. When comparing with the different MHT regimens, estrogen (E) + progesterone (P) regimen significantly increased TC (WMD: 0.15, 95% CI: 0.09 to 0.20), LDL-C (WMD: 0.12, 95% CI: 0.07-0.17) and Lp(a) (WMD: 44.58, 95% CI:28.09-61.06) compared with estrogen alone. Conclusion and Relevance: MHT plays a positive role in lipid profile in postmenopausal women, meanwhile for women with hypertriglyceridemia, low doses or transdermal MHT or tibolone would be a safer choice. Moreover, E + P regimen might blunt the benefit of estrogen on the lipid profile. Clinical Trial Registration: [https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42018092924], identifier [No. CRD42018092924].
Keywords: lipid profile; menopause hormone therapy; meta-analysis; postmenopausal women; system review.
Copyright © 2022 Nie, Yang, Wang, Liang, Li, Luo, Yang, Liu, Wang, Guo, Yu and Liang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Menopausal hormone therapy does not improve some domains of memory: A systematic review and meta-analysis.Front Endocrinol (Lausanne). 2022 Sep 6;13:894883. doi: 10.3389/fendo.2022.894883. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36147572 Free PMC article.
-
The benefits and risks of menopause hormone therapy for the cardiovascular system in postmenopausal women: a systematic review and meta-analysis.BMC Womens Health. 2024 Jan 23;24(1):60. doi: 10.1186/s12905-023-02788-0. BMC Womens Health. 2024. PMID: 38263123 Free PMC article.
-
The effects of exogenous estrogen in women with SAR-CoV-2 infection: a systematic review and meta-analysis.Hum Reprod. 2023 Jun 1;38(6):1111-1123. doi: 10.1093/humrep/dead074. Hum Reprod. 2023. PMID: 37071891
-
The effects of conjugated linoleic acid supplementation on lipid profile in adults: A systematic review and dose-response meta-analysis.Front Nutr. 2022 Nov 3;9:953012. doi: 10.3389/fnut.2022.953012. eCollection 2022. Front Nutr. 2022. PMID: 36438733 Free PMC article.
-
The effect of tibolone treatment on lipid profile in women: A systematic review and dose-response meta-analysis of randomized controlled trials.Pharmacol Res. 2021 Jul;169:105612. doi: 10.1016/j.phrs.2021.105612. Epub 2021 Apr 16. Pharmacol Res. 2021. PMID: 33865986
Cited by
-
Acute hyperlipidemia has transient effects on large-scale bone regeneration in male mice.Sci Rep. 2024 Oct 27;14(1):25610. doi: 10.1038/s41598-024-76992-9. Sci Rep. 2024. PMID: 39463386 Free PMC article.
-
Lipoprotein Metabolism, Dyslipidemia, and Lipid-Lowering Therapy in Women: A Comprehensive Review.Pharmaceuticals (Basel). 2024 Jul 9;17(7):913. doi: 10.3390/ph17070913. Pharmaceuticals (Basel). 2024. PMID: 39065763 Free PMC article. Review.
-
Availability of dietary secoisolariciresinol diglucoside on borderline blood cholesterol level in men: a randomized, parallel, controlled, double-blinded clinical trial.J Clin Biochem Nutr. 2024 May;74(3):261-266. doi: 10.3164/jcbn.23-122. Epub 2024 Mar 5. J Clin Biochem Nutr. 2024. PMID: 38799144 Free PMC article.
-
The Impact of Physical Activity on Metabolic Health and Cognitive Function in Postmenopausal Women: A Cross-Sectional Study.Metabolites. 2025 Jun 20;15(7):420. doi: 10.3390/metabo15070420. Metabolites. 2025. PMID: 40710520 Free PMC article.
-
High-Fat Diet and Metabolic Diseases: A Comparative Analysis of Sex-Dependent Responses and Mechanisms.Int J Mol Sci. 2025 May 16;26(10):4777. doi: 10.3390/ijms26104777. Int J Mol Sci. 2025. PMID: 40429918 Free PMC article. Review.
References
-
- Abbas A., Fadel P. J., Wang Z., Arbique D., Jialal I., Vongpatanasin W. (2004). Contrasting Effects of Oral versus Transdermal Estrogen on Serum Amyloid A (SAA) and High-Density Lipoprotein-SAA in Postmenopausal Women. Arterioscler Thromb. Vasc. Biol. 24 (10), e164–7. 10.1161/01.ATV.0000140198.16664.8e - DOI - PubMed
-
- Alomar S. A., Prabahar M. A. K., Arafah O. A., Almarshood F., Baradwan S., Aboudi S. A. S., et al. (2022). The Effect of Tamoxifen on the Lipid Profile in Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Exp. Gerontol. 159, 111680. 10.1016/j.exger.2021.111680 - DOI - PubMed
-
- Anagnostis P., Galanis P., Chatzistergiou V., Stevenson J. C., Godsland I. F., Lambrinoudaki I., et al. (2017). The Effect of Hormone Replacement Therapy and Tibolone on Lipoprotein (A) Concentrations in Postmenopausal Women: A Systematic Review and Meta-Analysis. Maturitas 99, 27–36. 10.1016/j.maturitas.2017.02.009 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous