

Kidney Transplant Outcomes of Patients With Multiple Myeloma
- PMID: 35497786
- PMCID: PMC9039485
- DOI: 10.1016/j.ekir.2022.01.003
Kidney Transplant Outcomes of Patients With Multiple Myeloma
Abstract
Introduction: Data on kidney transplantation (KTx) outcomes of patients with multiple myeloma (MM) are very limited.
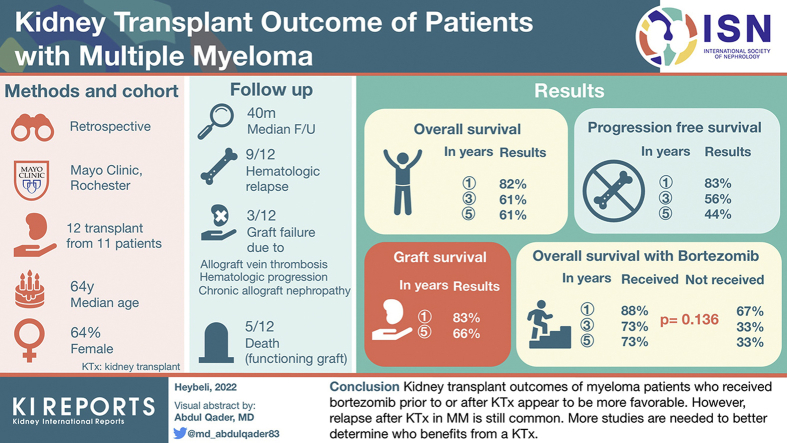
Methods: We investigated the outcomes of patients with MM who underwent KTx between 1994 and 2019.
Results: A total of 12 transplants from 11 patients were included. At the time of KTx, 6 were classified as having stringent complete response (CR), 2 as CR, 2 as very good partial response (VGPR), and 2 as partial response (PR). With a median follow-up of 40 (minimum-maximum, 5-92) months after KTx, hematologic progression occurred in 9 transplants (75%). There were 3 grafts (25%) that failed, and 5 patients (45.5%) experienced death with functioning allografts. Graft survival at 1 and 5 years was 82.5% and 66%, respectively. Progression-free survival (PFS) rates of the cohort at 1, 3, and 5 years were 83.3%, 55.6%, and 44.4%, respectively. The estimated median PFS of patients who received bortezomib at any time (pre-KTx and/or post-KTx) was not reached, whereas it was 24 months for those who never received bortezomib (P = 0.281). Overall survival (OS) rates of the cohort at 1, 3, and 5 years were 81.8%, 61.4%, and 61.4%, respectively. OS of patients who received bortezomib at any time was 87.5%, 72.9%, and 72.9%, and that for those who never received bortezomib was 66.7%, 33.3%, and 33.3% (P = 0.136). All deaths occurred owing to hematologic progression or treatment-related complications.
Conclusion: Kidney transplant outcomes of patients with myeloma who received bortezomib before or after KTx seem to be more favorable. Nevertheless, relapse after KTx in MM is still common. More studies are needed to better determine who benefits from a KTx.
Keywords: chronic kidney failure; graft survival; kidney transplantation; mortality; multiple myeloma; recurrence.
© 2022 International Society of Nephrology. Published by Elsevier Inc.
Figures



References
-
- Terpos E., Christoulas D., Kastritis E., et al. The Chronic Kidney Disease Epidemiology Collaboration cystatin C (CKD-EPI-CysC) equation has an independent prognostic value for overall survival in newly diagnosed patients with symptomatic multiple myeloma; is it time to change from MDRD to CKD-EPI-CysC equations? Eur J Haematol. 2013;91:347–355. doi: 10.1111/ejh.12164. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
