

Prediction of Incident Heart Failure in CKD: The CRIC Study
- PMID: 35497796
- PMCID: PMC9039424
- DOI: 10.1016/j.ekir.2022.01.1067
Prediction of Incident Heart Failure in CKD: The CRIC Study
Abstract
Introduction: Heart failure (HF) is common in chronic kidney disease (CKD); identifying patients with CKD at high risk for HF may guide clinical care. We assessed the prognostic value of cardiac biomarkers and echocardiographic variables for 10-year HF prediction compared with a published clinical HF prediction equation in a cohort of participants with CKD.
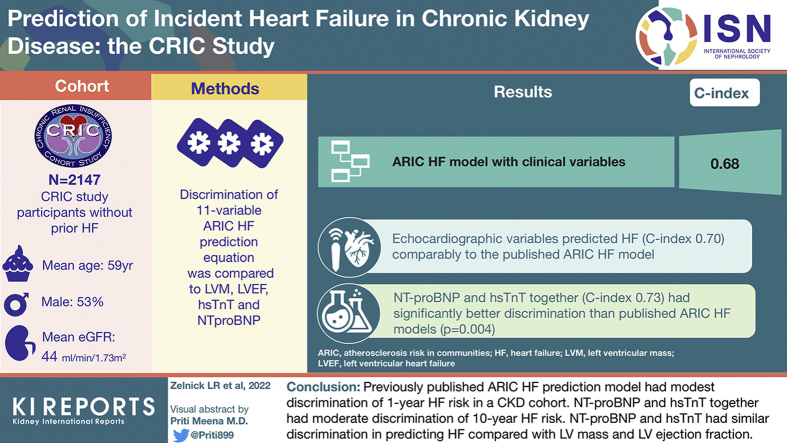
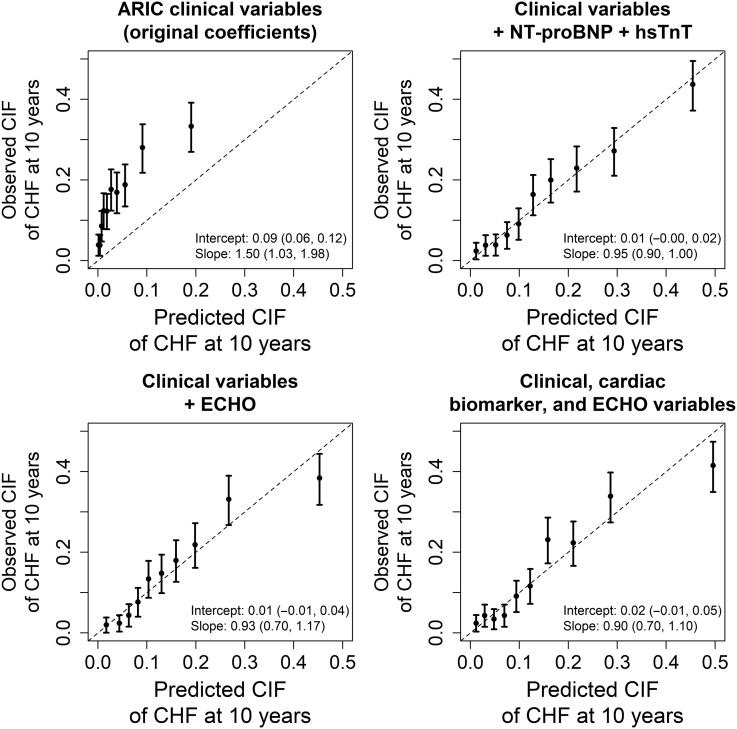
Methods: We studied 2147 Chronic Renal Insufficiency Cohort (CRIC) participants without prior HF with complete clinical, cardiac biomarker (N-terminal brain natriuretic peptide [NT-proBNP] and high sensitivity troponin-T [hsTnT]), and echocardiographic data (left ventricular mass [LVM] and left ventricular ejection fraction [LVEF] data). We compared the discrimination of the 11-variable Atherosclerosis Risk in Communities (ARIC) HF prediction equation with LVM, LVEF, hsTnT, and NT-proBNP to predict 10-year risk of hospitalization for HF using a Fine and Gray modeling approach. We separately evaluated prediction of HF with preserved and reduced LVEF (LVEF ≥50% and <50%, respectively). We assessed discrimination with internally valid C-indices using 10-fold cross-validation.
Results: Participants' mean (SD) age was 59 (11) years, 53% were men, 43% were Black, and mean (SD) estimated glomerular filtration rate (eGFR) was 44 (16) ml/min per 1.73 m2. A total of 324 incident HF hospitalizations occurred during median (interquartile range) 10.0 (5.7-10.0) years of follow-up. The ARIC HF model with clinical variables had a C-index of 0.68. Echocardiographic variables predicted HF (C-index 0.70) comparably to the published ARIC HF model, while NT-proBNP and hsTnT together (C-index 0.73) had significantly better discrimination (P = 0.004). A model including cardiac biomarkers, echocardiographic variables, and clinical variables had a C-index of 0.77. Discrimination of HF with preserved LVEF was lower than for HF with reduced LVEF for most models.
Conclusion: The ARIC HF prediction model for 10-year HF risk had modest discrimination among adults with CKD. NT-proBNP and hsTnT discriminated better than the ARIC HF model and at least as well as a model with echocardiographic variables. HF clinical prediction models tailored to adults with CKD are needed. Until then, measurement of NT-proBNP and hsTnT may be a low-burden approach to predicting HF in this population, as they offer moderate discrimination.
Keywords: biomarkers; cardiovascular disease; chronic kidney disease; echocardiogram; heart failure.
© 2022 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
