

Trends in Annual Incidence Rates of Newly Diagnosed Endomyocardial Fibrosis Cases at the Uganda Heart Institute: A 14-Year Review
- PMID: 35498040
- PMCID: PMC9051226
- DOI: 10.3389/fcvm.2022.841346
Trends in Annual Incidence Rates of Newly Diagnosed Endomyocardial Fibrosis Cases at the Uganda Heart Institute: A 14-Year Review
Abstract
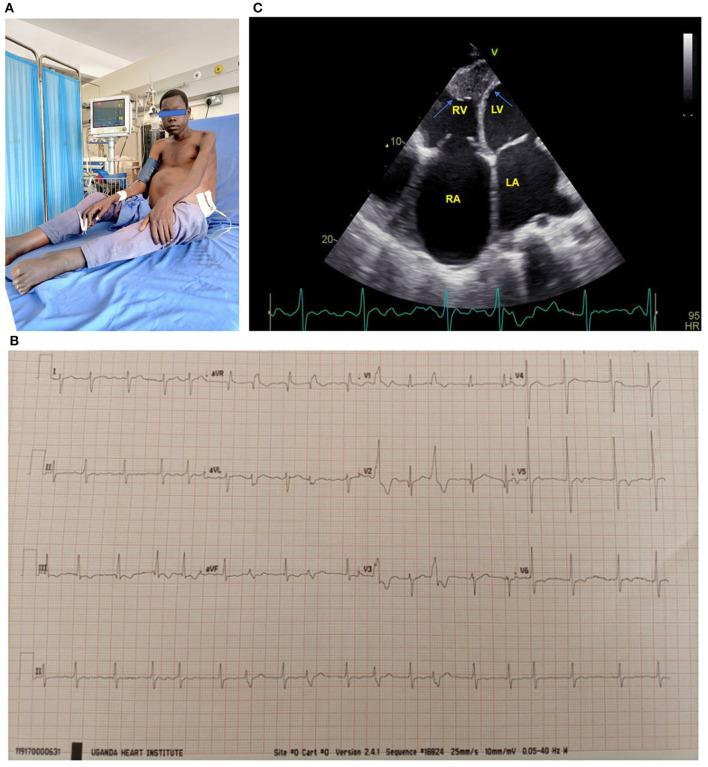
Background: First described in Uganda over seven decades ago, Endomyocardial fibrosis (EMF) is a rare form of restrictive cardiomyopathy found in the tropics. EMF occurs mainly in two phenotypes; biventricular involvement and right ventricular (RV) form. Previously endemic in several countries, there are reports suggesting that the disease is on the decline.
Objectives: To describe trends in annual incidence rates of newly diagnosed EMF cases at the Uganda Heart Institute (UHI).
Methods: This was a retrospective chart review of all newly diagnosed EMF cases at UHI from January 2007 to December 2020. Cases were divided into two groups A (2007-2013) and B (2014-2020).
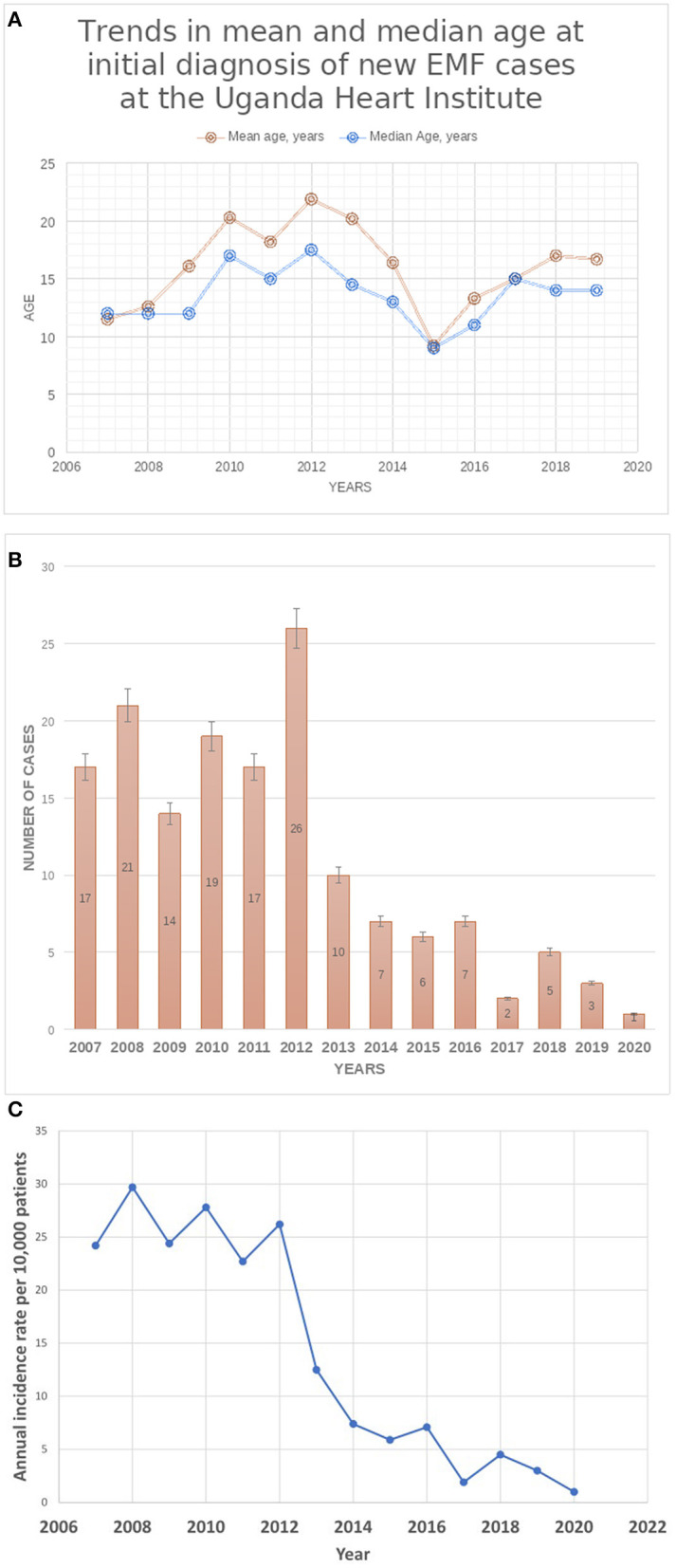
Results: A total of 155 cases were diagnosed during the period (Group A, n = 124; Group B, n = 31). There were no significant differences between the two groups A and B regarding median age at diagnosis (14 vs. 12 years, p = 0.0940), gender (48.4% female vs. 35.5%, p = 0.1987), and EMF type (66.9% RV EMF vs. 71.0%, p = 0.6634), respectively. The presence of complications such as intracardiac thrombus (5.6 vs. 32.2%, p = 0.0002) and pericardial effusion (57.3% vs. 80.6, p = 0.0172) were more frequent in group B than A, respectively. Pulmonary hypertension (PHT) was predominantly seen in cases with biventricular EMF compared to those with RV EMF (26 vs. 3.8%, p = 0.0001). The number of new cases diagnosed per year remained largely stable in the period 2007-2011, ranging 14-21 per year, peaked in 2012 (26 new cases), and thereafter declined from 10 cases seen in 2013 to 1-5 cases seen per year in the period 2017-2020. Similarly, the annual incidence rates of new EMF diagnosis remained relatively stable in the period 2007-2012, ranging between 22.7 and 29.7 per 10,000 patients seen in the echo labs, and then dramatically declined after 2012 to range between 1.0 and 4.5 new cases per 10,000 patients in the period between 2017 and 2020.
Conclusion: There has been a steady decline in the number of new cases of EMF seen at the UHI. However, there were no significant differences in the gender, age at diagnosis and EMF subtype of cases during the period under review. Complication rates were more frequent in the later cohort.
Keywords: Uganda; Uganda Heart Institute; endomyocardial fibrosis; incidence rates; trends.
Copyright © 2022 Aliku, Rwebembera, Lubega, Zhang, Lugero, Namuyonga, Omagino, Okello and Lwabi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Williams AW. Heart disease in the native population of Uganda. Part I: syphilitic heart disease. East Afr Med J. (1938) 15:279.
LinkOut - more resources
Full Text Sources