

Polypills for Primary Prevention of Cardiovascular Disease: A Systematic Review and Meta-Analysis
- PMID: 35498049
- PMCID: PMC9046936
- DOI: 10.3389/fcvm.2022.880054
Polypills for Primary Prevention of Cardiovascular Disease: A Systematic Review and Meta-Analysis
Abstract
Purpose: To evaluate the effect of polypills on the primary prevention of cardiovascular (CV) events using data from clinical trials.
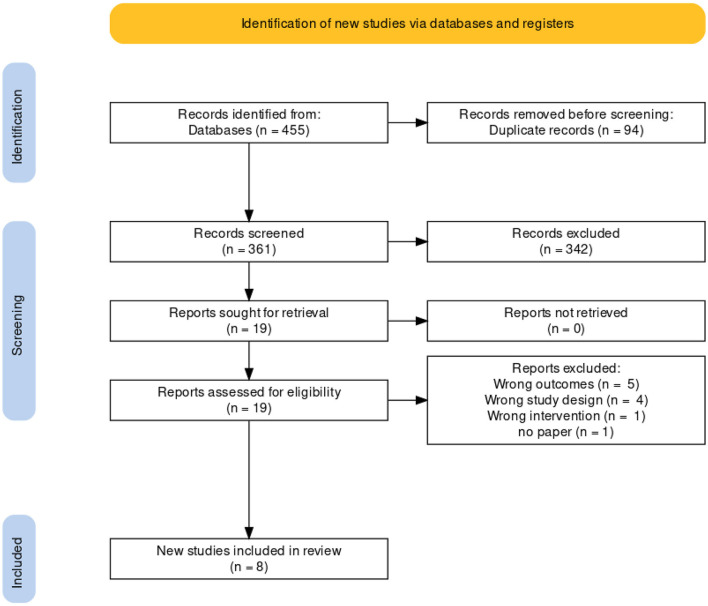
Methods: We searched PubMed, Web of Science, EBSCO, and SCOPUS throughout May 2021. Two authors independently screened articles for the fulfillment of inclusion criteria. The RevMan software (version 5.4) was used to calculate the pooled risk ratios (RRs) and mean differences (MDs), along with their associated confidence intervals (95% CI).
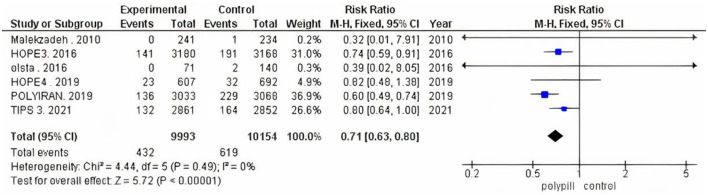
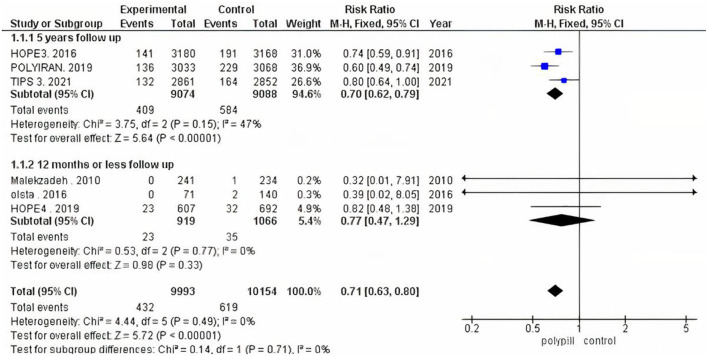
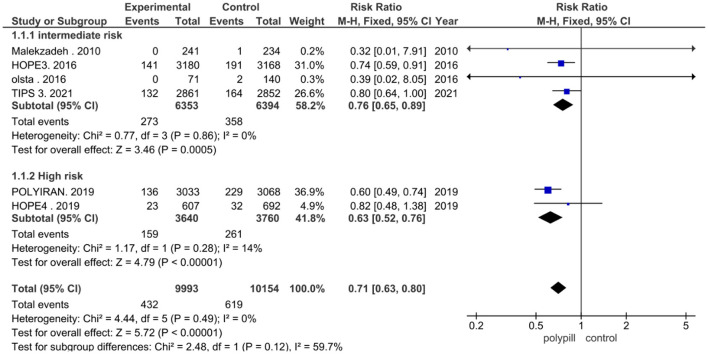
Results: Eight trials with a total of 20653 patients were included. There was a significant reduction in the total number of fatal and non-fatal CV events among the polypill group [RR (95% CI) = 0.71 (0.63, 0.80); P-value < 0.001]. This reduction was observed in both the intermediate-risk [RR (95% CI) = 0.76 (0.65, 0.89); P-value < 0.001] and high-risk [RR (95% CI) = 0.63 (0.52, 0.76); P-value < 0.001] groups of patients. Subgroup analysis was performed based on the follow-up duration of each study, and benefits were only evident in the five-year follow-up duration group [RR (95% CI) = 0.70 (0.62, 0.79); P-value < 0.001]. Benefits were absent in the one-year-or-less interval group [RR (95% CI) = 0.77 (0.47, 1.29); P-value = 0.330]. Additionally, there was a significant reduction in the 10-year predicted cardiovascular risk in the polypill group [MD (95% CI) = -3.74 (-5.96, -1.51); P-value < 0.001], as compared to controls.
Conclusion: A polypill regimen decreases the incidence of fatal and non-fatal CV events in patients with intermediate- and high- cardiovascular risk, and therefore may be an effective treatment for these patients.
Keywords: antihypertensives; cardiovascular events; lipid-lowering; polypill; primary prevention.
Copyright © 2022 Kandil, Motawea, Aboelenein and Shah.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Effect of the Polypill on Adherence and Prevention of Cardiovascular Diseases in Patients With or at High Risk of Cardiovascular Diseases: A Meta-Analysis of Randomized Controlled Trials.Cureus. 2023 Jan 24;15(1):e34134. doi: 10.7759/cureus.34134. eCollection 2023 Jan. Cureus. 2023. PMID: 36843692 Free PMC article. Review.
-
Meta-Analysis on the Clinical Outcomes With Polypills for Cardiovascular Disease Prevention.Am J Cardiol. 2023 Aug 15;201:211-218. doi: 10.1016/j.amjcard.2023.06.001. Epub 2023 Jun 27. Am J Cardiol. 2023. PMID: 37385176
-
Beta-blockers for suspected or diagnosed acute myocardial infarction.Cochrane Database Syst Rev. 2019 Dec 17;12(12):CD012484. doi: 10.1002/14651858.CD012484.pub2. Cochrane Database Syst Rev. 2019. PMID: 31845756 Free PMC article.
-
The Effectiveness of Polypill for the Prevention of Cardiovascular Disease: A Meta-Analysis of Randomized Controlled Trials.Cureus. 2023 Oct 14;15(10):e47032. doi: 10.7759/cureus.47032. eCollection 2023 Oct. Cureus. 2023. PMID: 38022292 Free PMC article. Review.
-
The effect of exposure to long working hours on stroke: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury.Environ Int. 2020 Sep;142:105746. doi: 10.1016/j.envint.2020.105746. Epub 2020 Jun 3. Environ Int. 2020. PMID: 32505015
Cited by
-
The Impact of Polypill on Adherence and Cardiovascular Outcomes: A Comprehensive Systematic Review with Meta-Analysis.Curr Cardiol Rev. 2024;20(2):61-71. doi: 10.2174/011573403X283174240110025442. Curr Cardiol Rev. 2024. PMID: 38265377 Free PMC article.
-
Adoption and scale-up of the cardiovascular Polypill: a realist institutional analysis.Health Policy Plan. 2023 Jan 6;38(1):15-27. doi: 10.1093/heapol/czac088. Health Policy Plan. 2023. PMID: 36271837 Free PMC article.
-
Efficacy of different polypill combinations for primary and secondary cardiovascular disease prevention: a systematic review and meta-analysis.Front Cardiovasc Med. 2025 Jun 9;12:1558579. doi: 10.3389/fcvm.2025.1558579. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40552187 Free PMC article.
-
Polypill protects MAFLD patients from cardiovascular events and mortality: a prospective trial.Hepatol Int. 2023 Aug;17(4):882-888. doi: 10.1007/s12072-023-10542-9. Epub 2023 May 25. Hepatol Int. 2023. PMID: 37227560 Clinical Trial.
References
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. . 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation. (2019) 140:e596–646. 10.1161/CIR.0000000000000678 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous