

Randomized clinical study to evaluate the effect of personalized therapy on patients with immunoglobulin A nephropathy
- PMID: 35498888
- PMCID: PMC9050523
- DOI: 10.1093/ckj/sfab263
Randomized clinical study to evaluate the effect of personalized therapy on patients with immunoglobulin A nephropathy
Erratum in
-
Erratum: Randomized clinical study to evaluate the effect of personalized therapy on patients with immunoglobulin A nephropathy.Clin Kidney J. 2022 Mar 12;15(5):1028. doi: 10.1093/ckj/sfac063. eCollection 2022 May. Clin Kidney J. 2022. PMID: 35503549 Free PMC article.
Abstract
Background: Randomized controlled trials (RCTs) have been conducted, stratifying idiopathic immunoglobulin A nephropathy (IgAN) patients based on the laboratory findings [serum creatinine, estimated glomerular filtration rate (eGFR) and daily proteinuria]. In contrast, data from kidney biopsy have been used only for clinical diagnosis. Therefore, IgAN patients with active or chronic renal lesions have been receiving the same therapy in experimental and control arms of randomized clinical trials (RCTs).
Methods: Our clinical study of IgAN (CLIgAN) is a multicentre, prospective, controlled and open-label RCT based on patients' stratification at the time of their kidney biopsy. We will consider, first, the type of renal lesions, followed by serum creatinine values, eGFR and proteinuria. Primary and secondary endpoints will be monitored. Then, we will determine whether personalized therapy can slow the decline of renal function and delay end-stage kidney disease.
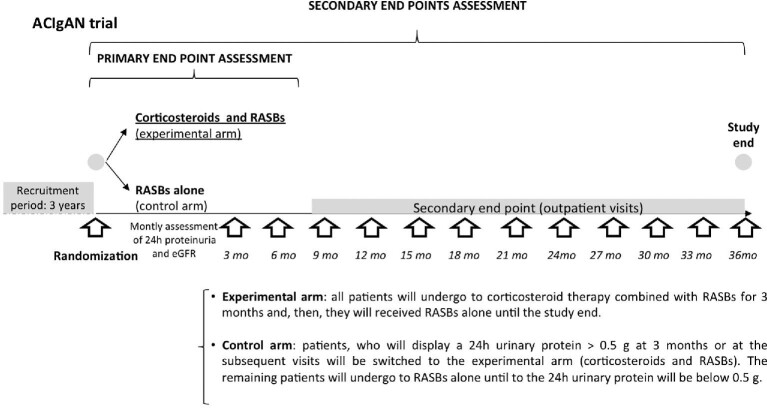
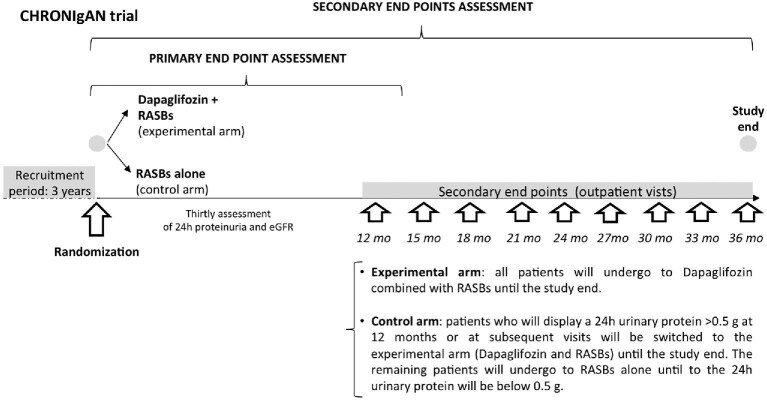
Results: We will enrol 132 IgAN patients with active renal lesions (66 patients per arm) in the first RCT (ACIgAN). They will receive corticosteroids combined with renin-angiotensin system blockers (RASBs) or only RASBs. A total of 294 IgAN patients with chronic or moderate renal lesions at high or very high risk of chronic kidney disease (147 patients per arm) will be enrolled in the second RCT (CHRONIgAN), in which they will receive dapagliflozin, a sodium-glucose cotransporter 2 inhibitor, combined with RASBs, or RASBs alone.
Conclusion: Using this approach, we hypothesize that patients could receive personalized therapy based on renal lesions to ensure that the right drug gets to the right patient at the right time.
Keywords: corticosteroids; dapagliflozin; immunoglobulin A nephropathy; kidney biopsy; randomized controlled trial; renin–angiotensin system blockers.
© The Author(s) 2021. Published by Oxford University Press on behalf of the ERA.
Figures

References
-
- Schena FP, Nistor I. Epidemiology of IgA nephropathy: a global perspective. Semin Nephrol 2018; 38: 435–442 - PubMed
-
- Koyama A, Igarashi M, Kobayashi M. Research Group on Progressive Renal Diseases. Natural history and risk factors for immunoglobulin A nephropathy in Japan. Am J Kidney Dis 1997; 29: 526–532 - PubMed
-
- Manno C, Strippoli GF, D'Altri Cet al. A novel simpler histological classification for renal survival in IgA nephropathy: a retrospective study. Am J Kidney Dis 2007; 49: 763–775 - PubMed
-
- KDIGO . KDIGO clinical practice guideline for glomerulonephritis. Kidney Int Suppl 2012; 2: 209–217
-
- Rovin BH, Adler SG, Barratt Jet al. Executive summary of the KDIGO 2021 guideline for the management of glomerular diseases. Kidney Int 2021; 100: 753–779 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
