

Efficacy and Safety of Fenfluramine for the Treatment of Seizures Associated With Lennox-Gastaut Syndrome: A Randomized Clinical Trial
- PMID: 35499850
- PMCID: PMC9062770
- DOI: 10.1001/jamaneurol.2022.0829
Efficacy and Safety of Fenfluramine for the Treatment of Seizures Associated With Lennox-Gastaut Syndrome: A Randomized Clinical Trial
Abstract
Importance: New treatment options are needed for patients with Lennox-Gastaut syndrome (LGS), a profoundly impairing, treatment-resistant, developmental and epileptic encephalopathy.
Objective: To evaluate the efficacy and safety of fenfluramine in patients with LGS.
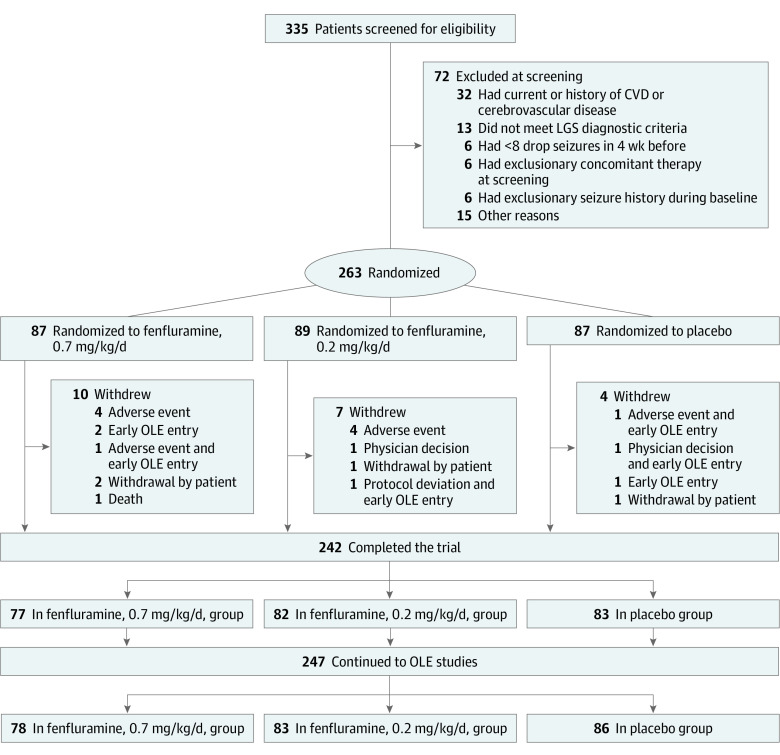
Design, setting, and participants: This multicenter, double-blind, placebo-controlled, parallel-group randomized clinical trial was conducted from November 27, 2017, to October 25, 2019, and had a 20-week trial duration. Patients were enrolled at 65 study sites in North America, Europe, and Australia. Included patients were aged 2 to 35 years with confirmed diagnosis of LGS and experienced 2 or more drop seizures per week during the 4-week baseline. Using a modified intent-to-treat method, data analysis was performed from November 27, 2017, to October 25, 2019. The database lock date was January 30, 2020, and the date of final report was September 11, 2021.
Interventions: Patients were randomized to receive either a 0.7-mg/kg/d or 0.2-mg/kg/d (maximum 26 mg/d) dose of fenfluramine or placebo. After titration (2-week period), patients were taking their randomized dose for 12 additional weeks.
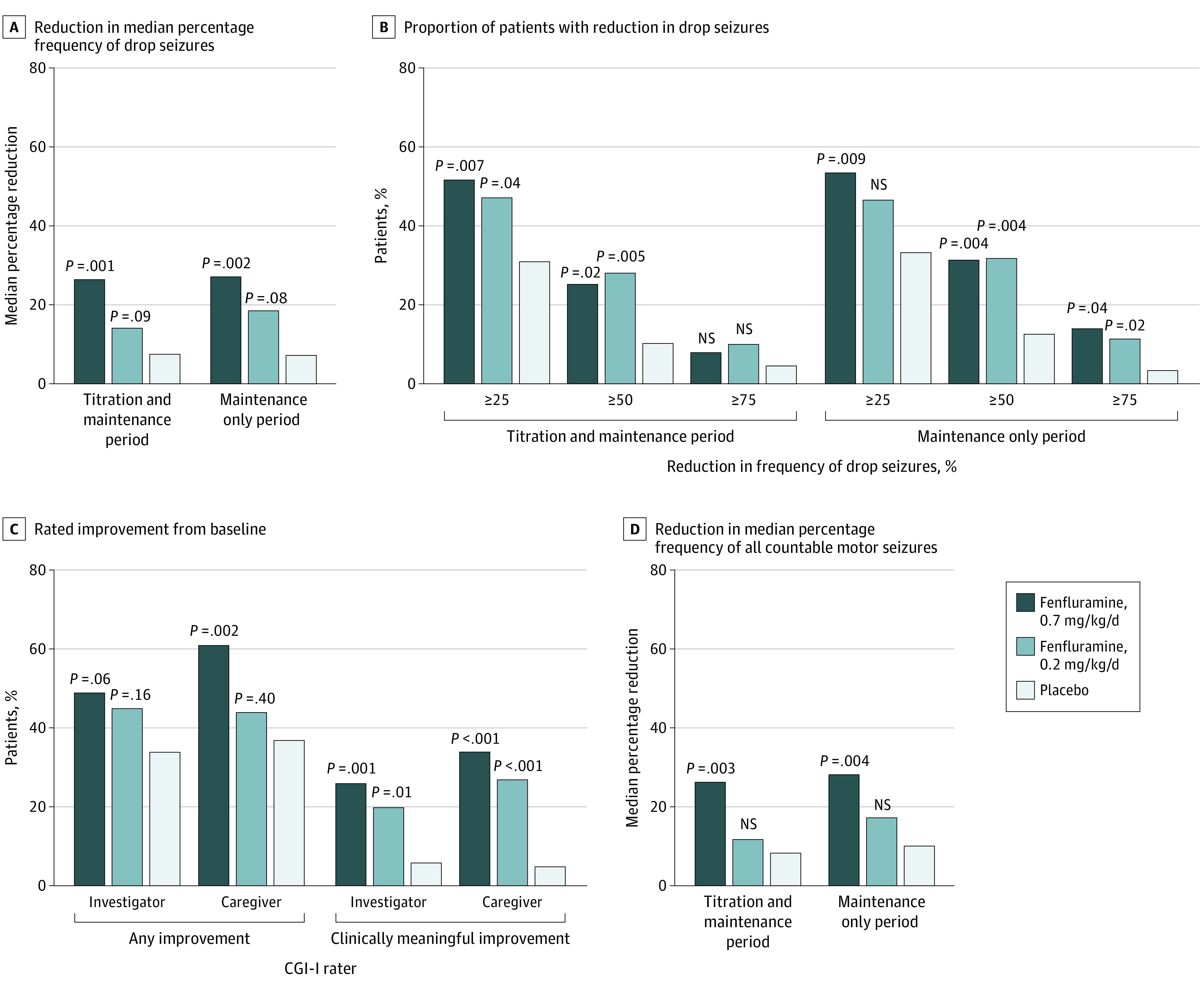
Main outcomes and measures: Primary efficacy end point was percentage change from baseline in drop seizure frequency in patients who received 0.7 mg/kg/d of fenfluramine vs placebo.
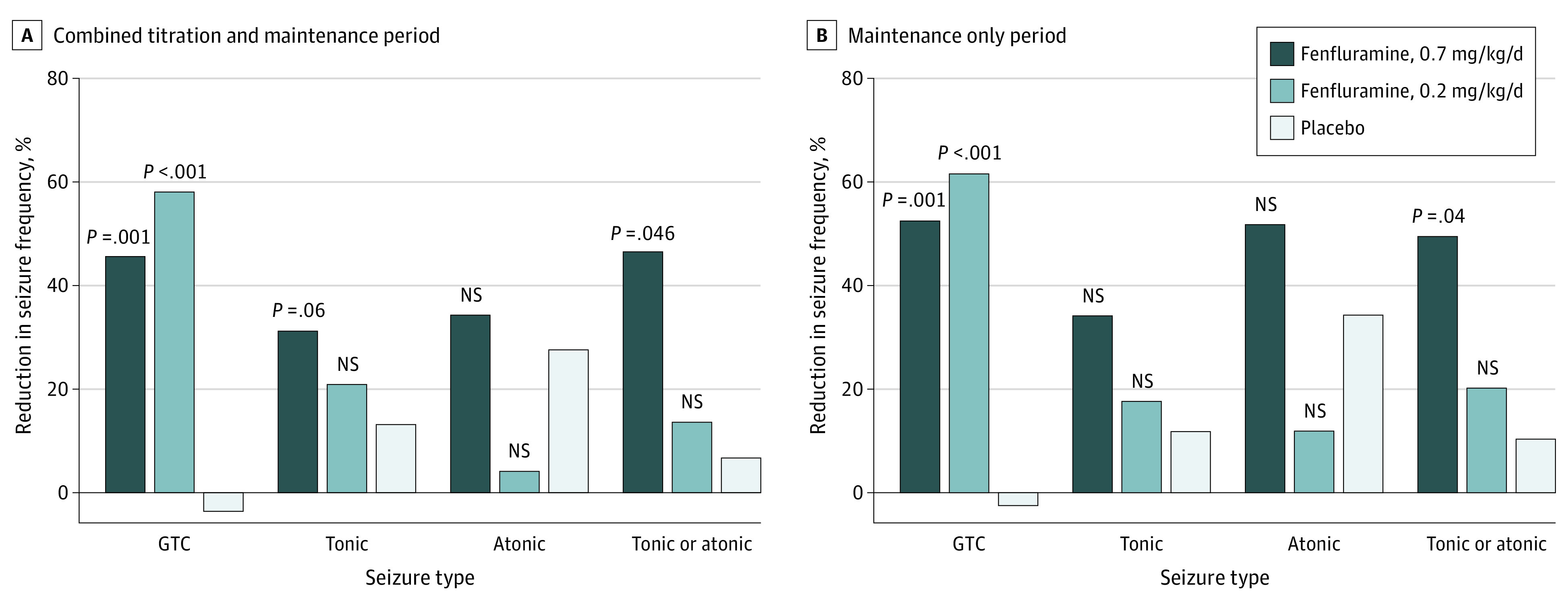
Results: A total of 263 patients (median [range] age, 13 [2-35] years; 146 male patients [56%]) were randomized to the 0.7-mg/kg/d fenfluramine group (n = 87), 0.2-mg/kg/d fenfluramine group (n = 89), or placebo group (n = 87). The median percentage reduction in frequency of drop seizures was 26.5 percentage points in the 0.7-mg/kg/d fenfluramine group, 14.2 percentage points in the 0.2-mg/kg/d fenfluramine group, and 7.6 percentage points in the placebo group. The trial met its primary efficacy end point: patients in the 0.7-mg/kg/d fenfluramine group achieved a -19.9 percentage points (95% CI, -31.0 to -8.7 percentage points; P = .001) estimated median difference in drop seizures from baseline vs placebo. More patients in the 0.7-mg/kg/d fenfluramine group achieved a 50% or greater response (22 of 87 [25%]; P = .02) vs placebo (9 of 87 [10%]). Site investigators and caregivers gave a much improved or very much improved rating on the Clinical Global Impression of Improvement scale to more patients in the 0.7-mg/kg/d fenfluramine group than patients in the placebo group (21 [26%] vs 5 [6%]; P = .001). The seizure subtype that appeared most responsive to fenfluramine was generalized tonic-clonic seizure (120 of 263 [46%]), with a decrease in frequency of 45.7% in the 0.7-mg/kg/d fenfluramine group and 58.2% in the 0.2-mg/kg/d fenfluramine group compared with an increase of 3.7% in the placebo group. Most common treatment-emergent adverse events included decreased appetite (59 [22%]), somnolence (33 [13%]), and fatigue (33 [13%]). No cases of valvular heart disease or pulmonary arterial hypertension were observed.
Conclusions and relevance: Results of this trial showed that, in patients with LGS, fenfluramine compared with placebo provided a significantly greater reduction in drop seizures and may be a particularly advantageous choice in patients who experience generalized tonic-clonic seizures.
Trial registration: ClinicalTrials.gov Identifier: NCT03355209.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
