

Metastatic Death Based on Presenting Features and Treatment for Advanced Intraocular Retinoblastoma: A Multicenter Registry-Based Study
- PMID: 35500608
- PMCID: PMC9329221
- DOI: 10.1016/j.ophtha.2022.04.022
Metastatic Death Based on Presenting Features and Treatment for Advanced Intraocular Retinoblastoma: A Multicenter Registry-Based Study
Abstract
Purpose: To evaluate presenting features, tumor size, and treatment methods for risk of metastatic death due to advanced intraocular retinoblastoma (RB).
Design: International, multicenter, registry-based retrospective case series.
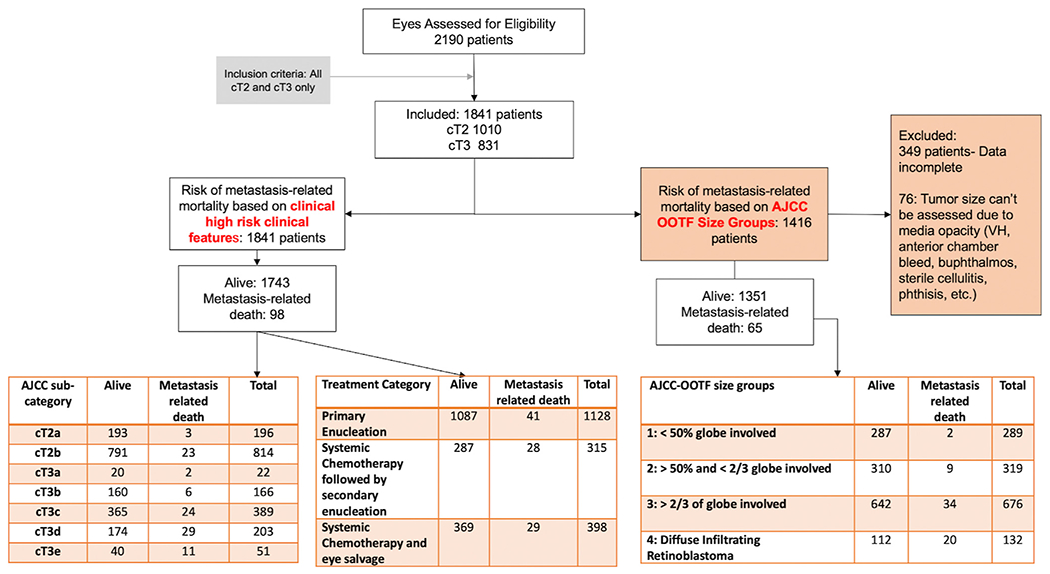
Participants: A total of 1841 patients with advanced RB.
Methods: Advanced RB was defined by 8th edition American Joint Committee on Cancer (AJCC) categories cT2 and cT3 and new AJCC-Ophthalmic Oncology Task Force (OOTF) Size Groups (1: < 50% of globe volume, 2: > 50% but < 2/3, 3: > 2/3, and 4: diffuse infiltrating RB). Treatments were primary enucleation, systemic chemotherapy with secondary enucleation, and systemic chemotherapy with eye salvage.
Main outcome measures: Metastatic death.
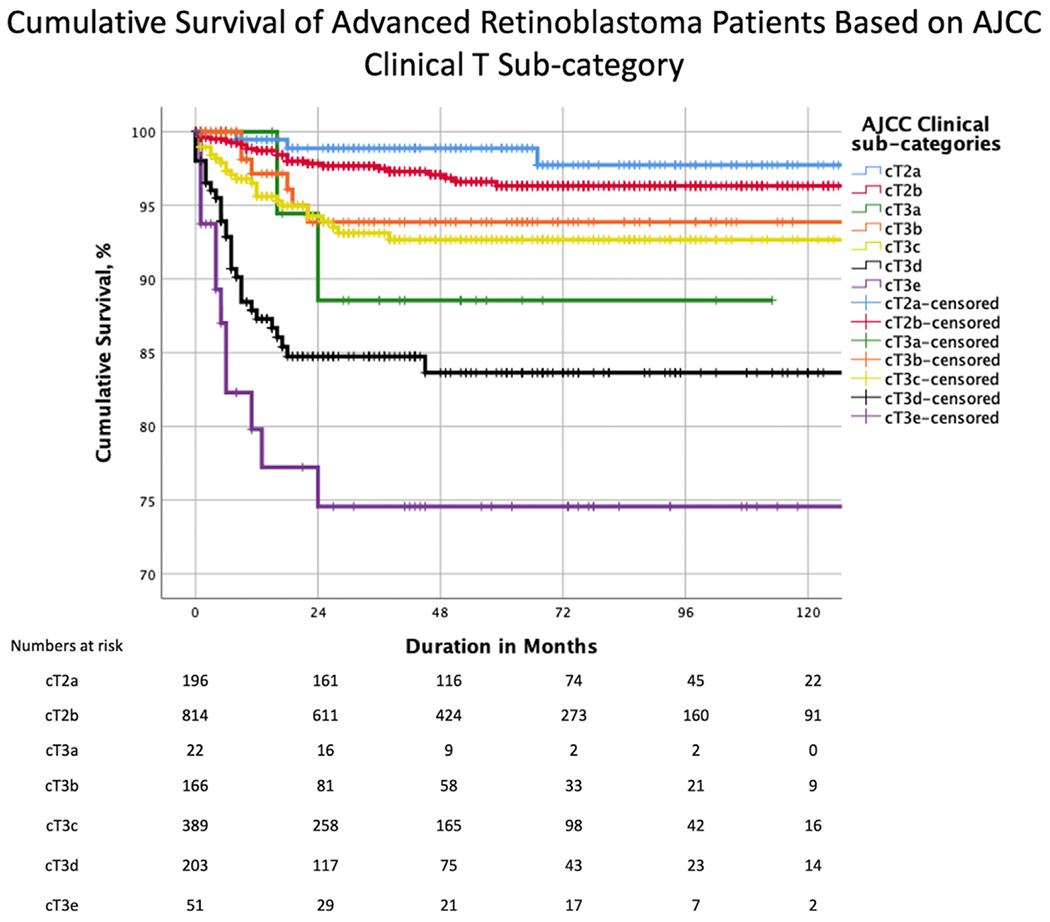
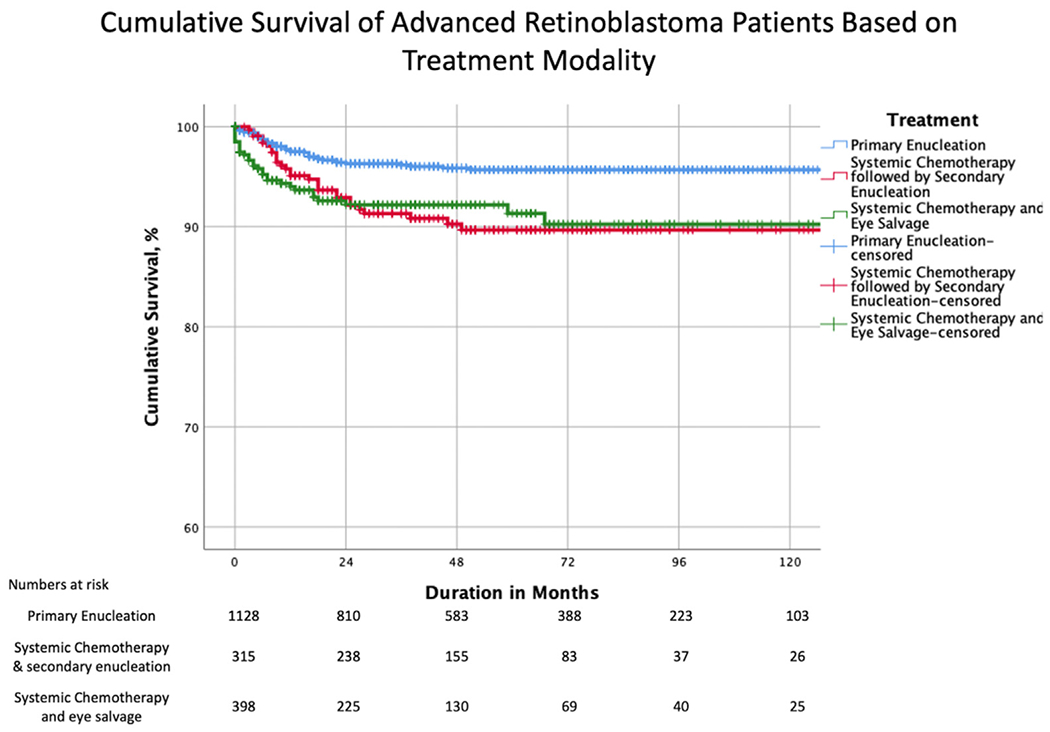
Results: The 5-year Kaplan-Meier cumulative survival estimates by patient-level AJCC clinical subcategories were 98% for cT2a, 96% for cT2b, 88% for cT3a, 95% for cT3b, 92% for cT3c, 84% for cT3d, and 75% for cT3e RB. Survival estimates by treatment modality were 96% for primary enucleation, 89% for systemic chemotherapy and secondary enucleation, and 90% for systemic chemotherapy with eye salvage. Risk of metastatic mortality increased with increasing cT subcategory (P < 0.001). Cox proportional hazards regression analysis confirmed a higher risk of metastatic mortality in categories cT3c (glaucoma, hazard ratio [HR], 4.9; P = 0.011), cT3d (intraocular hemorrhage, HR, 14.0; P < 0.001), and cT3e (orbital cellulitis, HR, 19.6; P < 0.001) than in category cT2a and with systemic chemotherapy with secondary enucleation (HR, 3.3; P < 0.001) and eye salvage (HR, 4.9; P < 0.001) than with primary enucleation. The 5-year Kaplan-Meier cumulative survival estimates by AJCC-OOTF Size Groups 1 to 4 were 99%, 96%, 94%, and 83%, respectively. Mortality from metastatic RB increased with increasing Size Group (P < 0.001). Cox proportional hazards regression analysis revealed that patients with Size Group 3 (HR, 10.0; P = 0.002) and 4 (HR, 41.1; P < 0.001) had a greater risk of metastatic mortality than Size Group 1.
Conclusions: The AJCC-RB cT2 and cT3 subcategories and size-based AJCC-OOTF Groups 3 (> 2/3 globe volume) and 4 (diffuse infiltrating RB) provided a robust stratification of clinical risk for metastatic death in advanced intraocular RB. Primary enucleation offered the highest survival rates for patients with advanced intraocular RB.
Keywords: AJCC; Advanced; Chemotherapy; Enucleation; International; Metastasis; Multicenter; Registry; Retinoblastoma; Staging.
Copyright © 2022 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Re: Tomar et al.: American Joint Committee on Cancer Ophthalmic Oncology Task Force. High-risk pathologic features based on presenting findings in advanced intraocular retinoblastoma: a multicenter, international data-sharing American Joint Committee on Cancer Study (Ophthalmology. 2022;129:923-932) and Tomar et al.: American Joint Committee on Cancer Ophthalmic Oncology Task Force. Metastatic death based on presenting features and treatment for advanced intraocular retinoblastoma: a multicenter registry-based study. (Ophthalmology. 2022;129:933-945).Ophthalmology. 2023 Mar;130(3):e11-e12. doi: 10.1016/j.ophtha.2022.10.018. Epub 2022 Nov 25. Ophthalmology. 2023. PMID: 36443123 No abstract available.
References
-
- Finger PT. Do you speak ocular tumor? Ophthalmology. 2003;110:13–14. - PubMed
-
- Finger PT. Foundational elements for collaboration in ophthalmic oncology. Ophthalmol Retina. 2017;1:263–265. - PubMed
-
- Kletke SN, Feng ZX, Hazrati LN, et al. Clinical predictors at diagnosis of low-risk histopathology in unilateral advanced retinoblastoma. Ophthalmology. 2019;126:1306–1314. - PubMed
-
- Munier FL, Beck-Popovic M, Chantada GL, et al. Conservative management of retinoblastoma: challenging orthodoxy without compromising the state of metastatic grace. “Alive, with good vision and no comorbidity.”. Prog Retin Eye Res. 2019;73: 100764. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
