

Transferring neurointerventionalists saves time compared with interhospital transfer of stroke patients for endovascular thrombectomy: a collaborative pooled analysis of 1001 patients (EVEREST)
- PMID: 35501118
- PMCID: PMC10313980
- DOI: 10.1136/neurintsurg-2021-018049
Transferring neurointerventionalists saves time compared with interhospital transfer of stroke patients for endovascular thrombectomy: a collaborative pooled analysis of 1001 patients (EVEREST)
Abstract
Background: Interhospital transfer of stroke patients (drip and ship concept) is associated with longer treatment times compared with primary admission to a comprehensive stroke center (mothership concept). In recent years, studies on a novel concept of performing endovascular thrombectomy (EVT) at external hospitals (EXT) by transferring neurointerventionalists, instead of patients, have been published. This collaborative study aimed at answering the question of whether EXT saves time in the workflow of acute stroke treatment across various geographical regions.
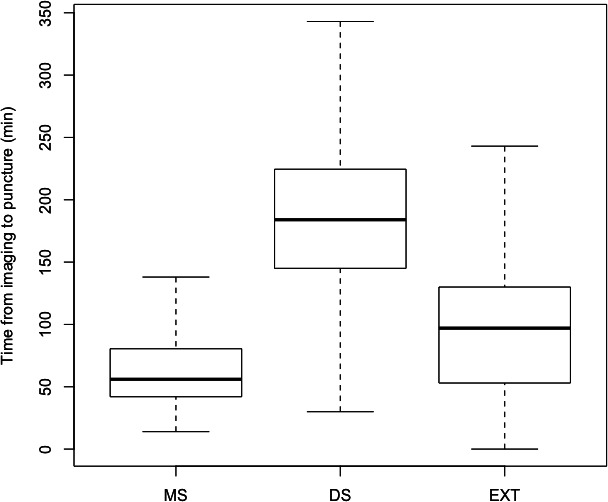
Methods: This was a patient level pooled analysis of one prospective observational study and four retrospective cohort studies, the EVEREST collaboration (EndoVascular thrombEctomy at Referring and External STroke centers). Time from initial stroke imaging to EVT (vascular puncture) was compared in mothership, drip and ship, and EXT concepts.
Results: In total, 1001 stroke patients from various geographical regions who underwent EVT due to large vessel occlusion were included. These were divided into mothership (n=162, 16.2%), drip and ship (n=458, 45.8%), and EXT (n=381, 38.1%) cohorts. The median time periods from onset to EVT (195 min vs 320 min, p<0.001) and from imaging to EVT (97 min vs 184 min, p<0.001) in EXT were significantly shorter than for drip and ship thrombectomy concept.
Conclusions: This pooled analysis of the EVEREST collaboration adds evidence that performing EVT at external hospitals can save time compared with drip and ship across various geographical regions. We encourage conducting randomized controlled trials comparing both triage concepts.
Keywords: Stroke; Thrombectomy.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: FS: research support from Stryker and member of the editorial board of JNIS. JF: research support from German Ministry of Science and Education (BMBF), German Ministry of Economy and Innovation (BMWi), German Research Foundation (DFG), European Union (EU), Hamburgische Investitions-und Förderbank (IFB), Medtronic, Microvention, Philips, and Stryker; consultant for Acandis, Boehringer Ingelheim, Cerenovus, Covidien, Evasc Neurovascular, MD Clinicals, Medtronic, Medina, Microvention, Penumbra, Route92, Stryker, and Transverse Medical; and member of the editorial board of JNIS. MAM: unrelated: board membership of Codman; consultancy for Medtronic, MicroVention, and Stryker; grants/grants pending from Balt, and MicroVention (money paid to the institution); payment for lectures including service on speakers bureaus for Medtronic, MicroVention, and Stryker. MB: (all unrelated): research support from Stryker, European Union, DFG, Hopp Foundation, Novartis, and Siemens; consultancy for Vascular Dynamics, Boehringer, and BBraun; personal fees from Novartis, Grifols, Merck, TEVA and Bayer.
Figures
Similar articles
-
Drip-and-ship toward mothership model for mechanical thrombectomy during COVID-19 pandemic: a retrospective analysis.Neurol Sci. 2023 Jan;44(1):1-7. doi: 10.1007/s10072-022-05903-5. Epub 2022 Jan 31. Neurol Sci. 2023. PMID: 35099642 Free PMC article.
-
Two Paradigms for Endovascular Thrombectomy After Intravenous Thrombolysis for Acute Ischemic Stroke.JAMA Neurol. 2017 May 1;74(5):549-556. doi: 10.1001/jamaneurol.2016.5823. JAMA Neurol. 2017. PMID: 28319240 Free PMC article.
-
Clinical Outcome After Endovascular Thrombectomy in 3 Triage Concepts: A Prospective, Observational Study (NEUROSQUAD).Stroke. 2021 Jun;52(6):e213-e216. doi: 10.1161/STROKEAHA.120.030520. Epub 2021 Apr 29. Stroke. 2021. PMID: 33910365
-
Pathway Design for Acute Stroke Care in the Era of Endovascular Thrombectomy: A Critical Overview of Optimization Efforts.Stroke. 2020 Nov;51(11):3452-3460. doi: 10.1161/STROKEAHA.120.030392. Epub 2020 Oct 19. Stroke. 2020. PMID: 33070713 Review.
-
Mothership versus drip and ship for thrombectomy in patients who had an acute stroke: a systematic review and meta-analysis.J Neurointerv Surg. 2019 Jan;11(1):14-19. doi: 10.1136/neurintsurg-2018-014249. Epub 2018 Oct 8. J Neurointerv Surg. 2019. PMID: 30297541
Cited by
-
Interfacility Transfer for Thrombectomy: A Promising Therapeutic Window.Stroke. 2025 Feb;56(2):564-574. doi: 10.1161/STROKEAHA.124.049167. Epub 2024 Nov 6. Stroke. 2025. PMID: 39502034 Review.
References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. . Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019;50:e344–418. 10.1161/STR.0000000000000211 - DOI - PubMed
-
- Jauch EC, Schwamm LH, Panagos PD, et al. . Recommendations for regional stroke destination plans in rural, suburban, and urban communities from the prehospital stroke system of care consensus conference: a consensus statement from the American Academy of Neurology, American Heart Association/American Stroke Association, American Society of Neuroradiology, National Association of EMS Physicians, National Association of State EMS Officials, Society of NeuroInterventional Surgery, and Society of Vascular and Interventional Neurology: endorsed by the Neurocritical Care Society. Stroke 2021;52:e133–52. 10.1161/STROKEAHA.120.033228 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical