

Screening for Colorectal Cancer
- PMID: 35501176
- PMCID: PMC9167799
- DOI: 10.1016/j.hoc.2022.02.001
Screening for Colorectal Cancer
Abstract
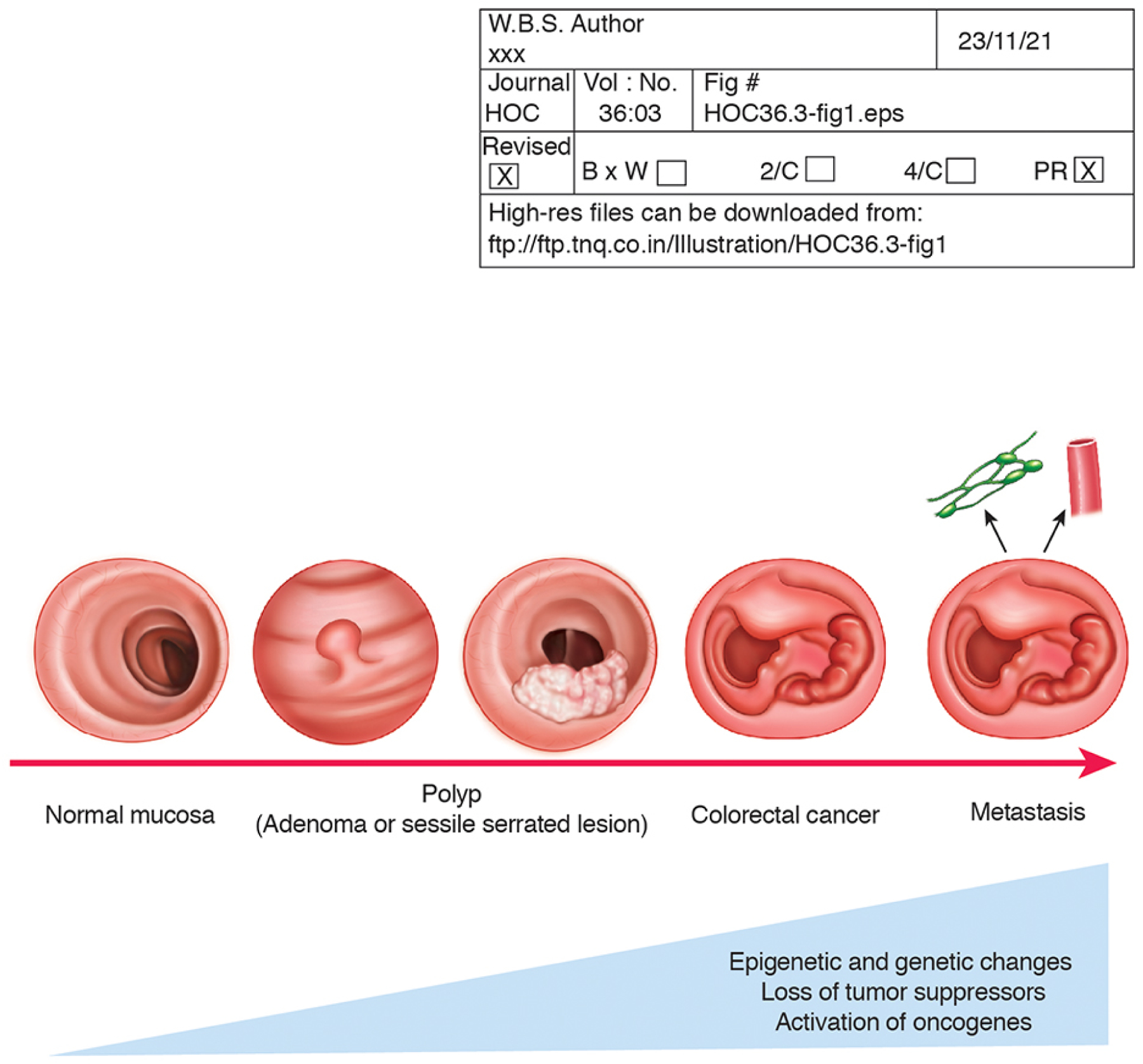
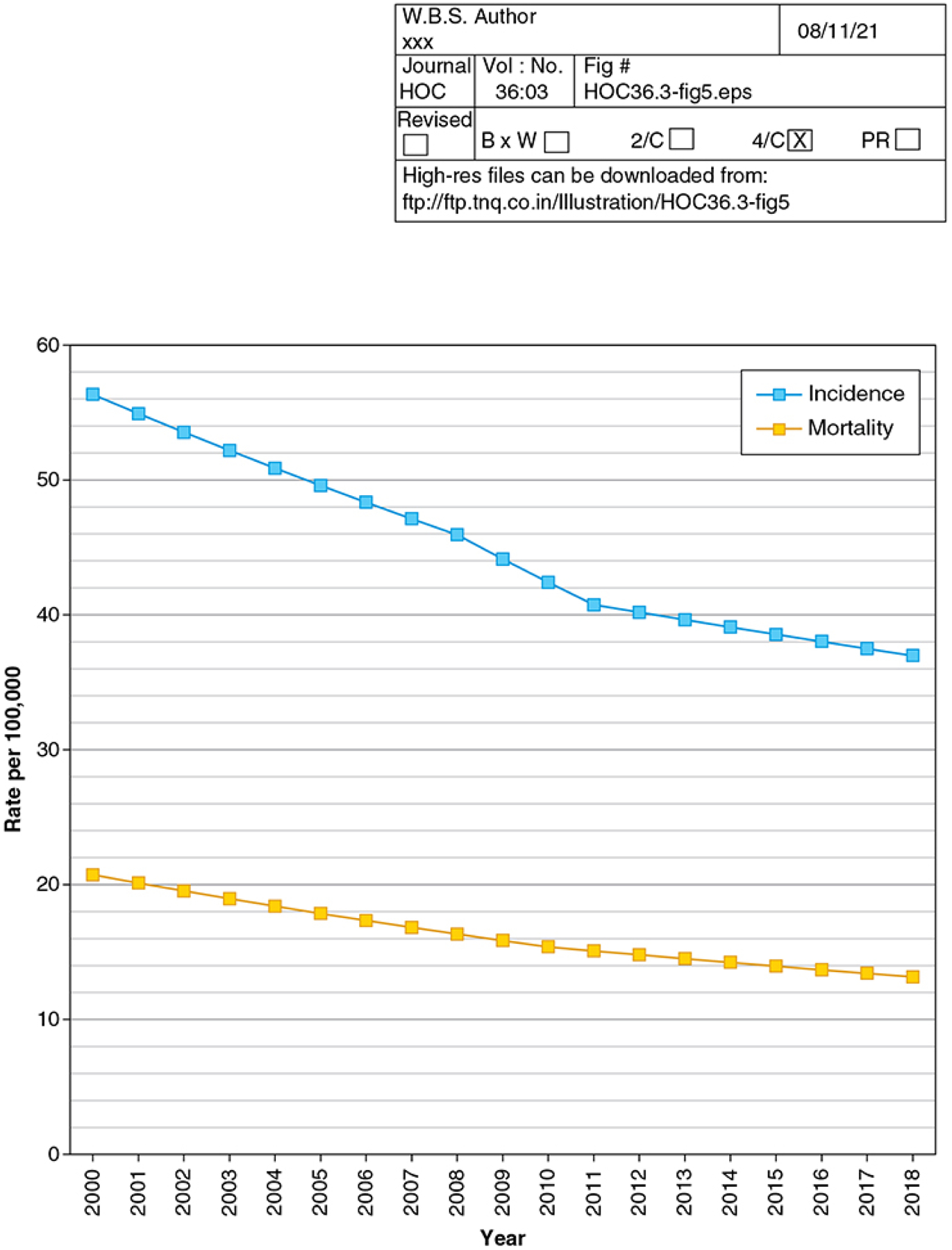
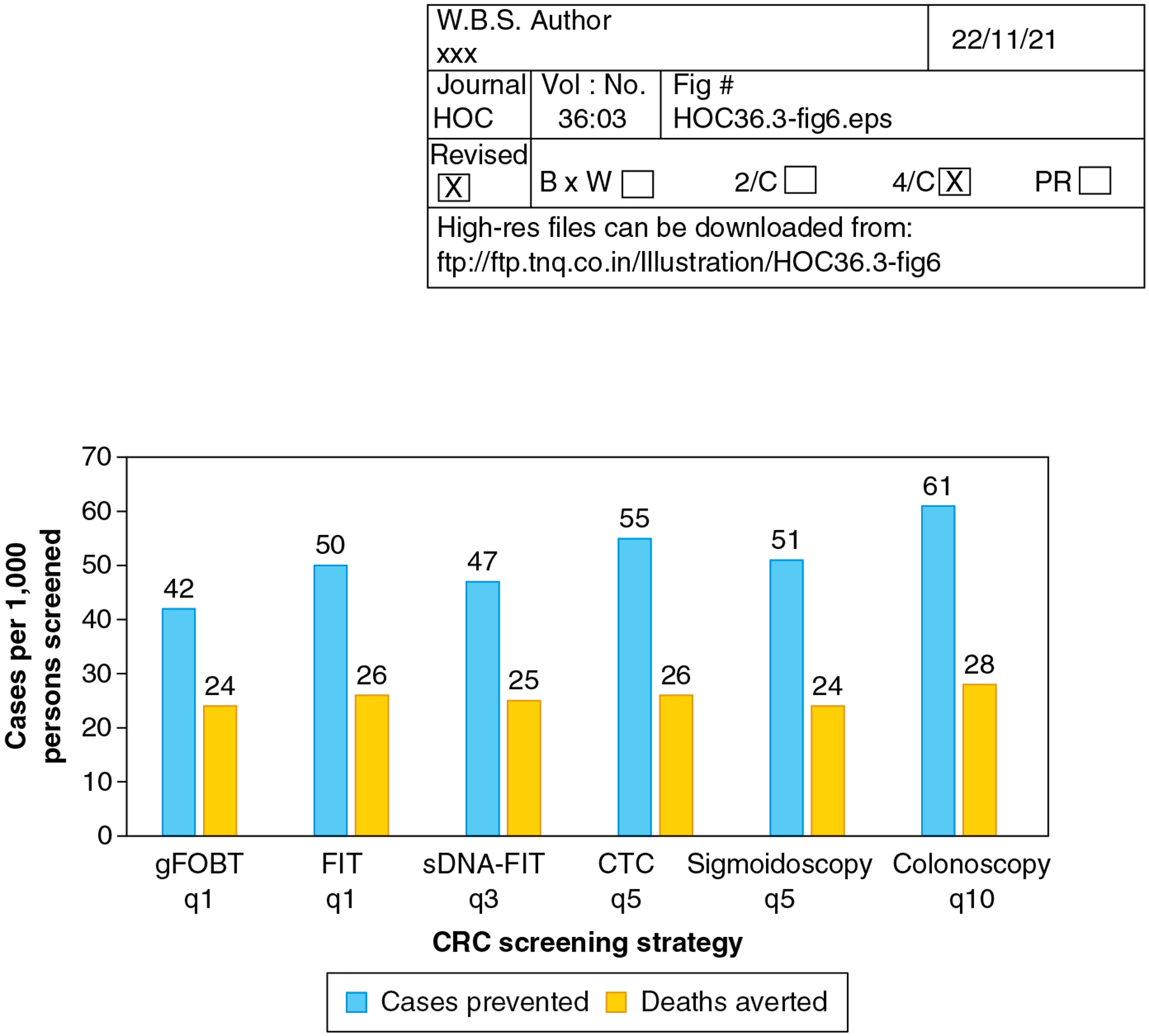
Colorectal cancer (CRC) is the second-leading cause of cancer death in the United States. Screening reduces CRC incidence and mortality. 2021 US Preventive Service Task Force (USPSTF) guidelines and available evidence support routine screening from ages 45 to 75, and individualized consideration of screening ages 76 to 85. USPSTF guidelines recommend annual guaiac fecal occult blood testing, annual fecal immunochemical testing (FIT), annual to every 3-year multitarget stool DNA-FIT, every 5-year sigmoidoscopy, every 10-year sigmoidoscopy with annual FIT, every 5-year computed tomographic colonography, and every 10-year colonoscopy as options for screening. The "best test is the one that gets done."
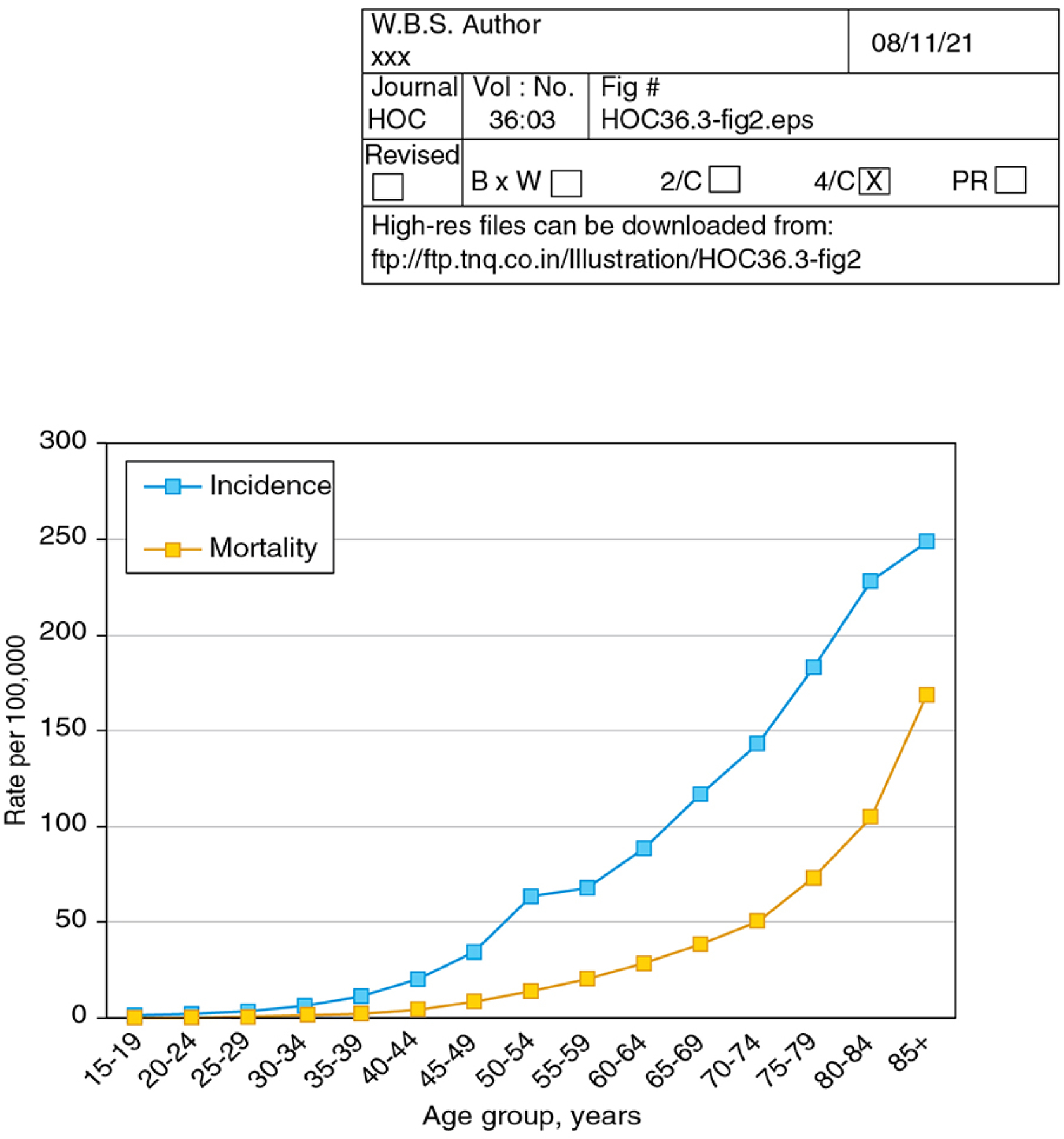
Keywords: Colorectal cancer; Early detection; Incidence; Mortality; Prevention; Screening.
Published by Elsevier Inc.
Conflict of interest statement
Disclosure The author serves as a local site investigator for 2 trials investigating blood-based biomarkers for colorectal cancer screening sponsored by Freenome Holdings, Inc and Epigenomics AG. The author serves as a paid consultant to Guardant Health and CellMax Life, which are developing blood-based biomarkers for colorectal cancer screening.
Figures

References
-
- Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA: A Cancer Journal for Clinicians. 2020;0:1–20. - PubMed
-
- Colon and Rectum SEER Incidence and U.S. Mortality Rates by Age at Diagnosis, 2014–2018. In: SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance, Epidemiology, and End Results Program, National Cancer Institute. Available at:https://seer.cancer.gov/explorer/application.html?site=20&data_type=9&gr.... Accessed August 27, 2021.
-
- Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394(10207):1467–1480. - PubMed
-
- Risk factors and protective factors. In: IARC (2019). Colorectal cancer screening. IARC Handb Cancer Prev. 17:1–300. Available from: http://publications.iarc.fr/573.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
