

Cerebellar Transcranial Direct Current Stimulation in Spinocerebellar Ataxia Type 3: a Randomized, Double-Blind, Sham-Controlled Trial
- PMID: 35501469
- PMCID: PMC9059914
- DOI: 10.1007/s13311-022-01231-w
Cerebellar Transcranial Direct Current Stimulation in Spinocerebellar Ataxia Type 3: a Randomized, Double-Blind, Sham-Controlled Trial
Abstract
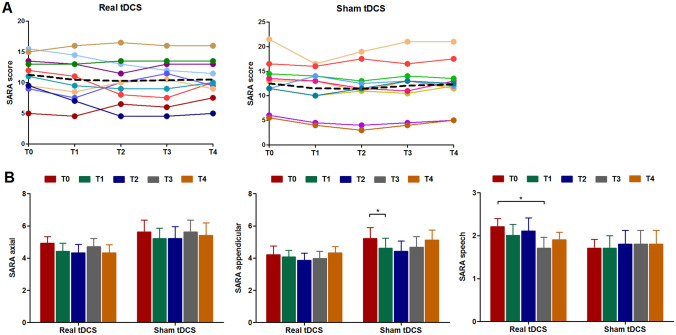
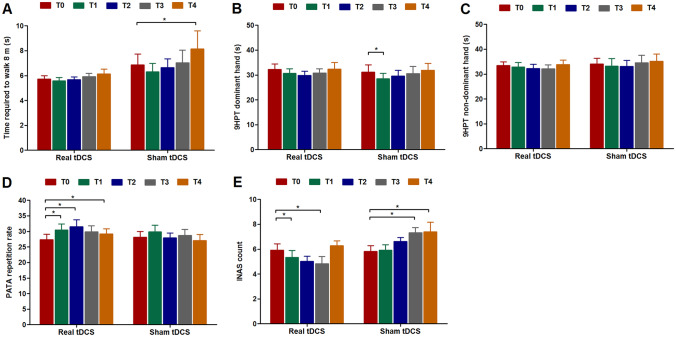
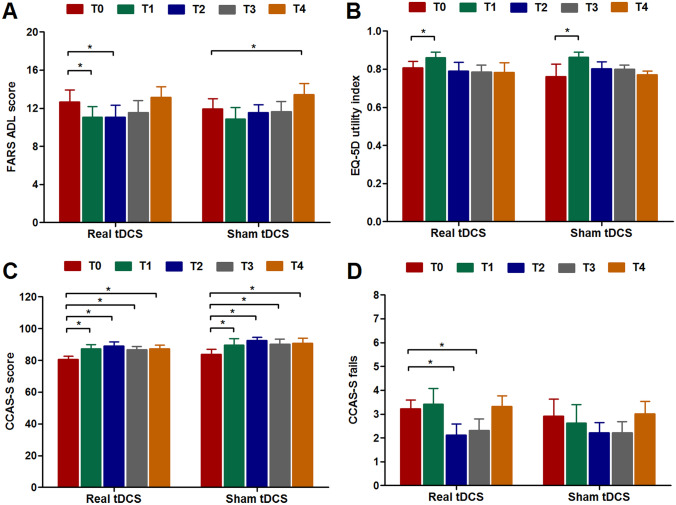
Repeated sessions of cerebellar anodal transcranial direct current stimulation (tDCS) have been suggested to modulate cerebellar-motor cortex (M1) connectivity and decrease ataxia severity. However, therapeutic trials involving etiologically homogeneous groups of ataxia patients are lacking. The objective of this study was to investigate if a two-week regimen of daily cerebellar tDCS sessions diminishes ataxia and non-motor symptom severity and alters cerebellar-M1 connectivity in individuals with spinocerebellar ataxia type 3 (SCA3). We conducted a randomized, double-blind, sham-controlled trial in which twenty mildly to moderately affected SCA3 patients received ten sessions of real or sham cerebellar tDCS (i.e., five days per week for two consecutive weeks). Effects were evaluated after two weeks, three months, six months, and twelve months. Change in Scale for the Assessment and Rating of Ataxia (SARA) score after two weeks was defined as the primary endpoint. Static posturography, SCA Functional Index tests, various patient-reported outcome measures, the cerebellar cognitive affective syndrome scale, and paired-pulse transcranial magnetic stimulation to examine cerebellar brain inhibition (CBI) served as secondary endpoints. Absolute change in SARA score did not differ between both trial arms at any of the time points. We observed significant short-term improvements in several motor, cognitive, and patient-reported outcomes after the last stimulation session in both groups but no treatment effects in favor of real tDCS. Nonetheless, some of the patients in the intervention arm showed a sustained reduction in SARA score lasting six or even twelve months, indicating interindividual variability in treatment response. CBI, which reflects the functional integrity of the cerebellothalamocortical tract, remained unchanged after ten tDCS sessions. Albeit exploratory, there was some indication for between-group differences in SARA speech score after six and twelve months and in the number of extracerebellar signs after three and six months. Taken together, our study does not provide evidence that a two-week treatment with daily cerebellar tDCS sessions reduces ataxia severity or restores cerebellar-M1 connectivity in early-to-middle-stage SCA3 patients at the group level. In order to potentially increase therapeutic efficacy, further research is warranted to identify individual predictors of symptomatic improvement.
Keywords: Cerebellar brain inhibition; Randomized controlled trial; Scale for the Assessment and Rating of Ataxia; Spinocerebellar ataxia type 3; Transcranial direct current stimulation; Transcranial magnetic stimulation.
© 2022. The Author(s).
Conflict of interest statement
Roderick Maas, Steven Teerenstra, Ivan Toni, and Dennis Schutter report no disclosures. Thomas Klockgether receives or has received research support from the Deutsche Forschungsgemeinschaft (DFG), the Bundesministerium für Bildung und Forschung (BMBF), the Bundesministerium für Gesundheit (BMG), the Robert Bosch Foundation, the European Union (EU), and the National Institutes of Health (NIH). He has received consulting fees from Biohaven, uniQure, Vico Therapeutics, Roche, and UBC. He has received a speaker honorarium from Novartis and Bayer. Bart van de Warrenburg receives research support from ZonMw, Hersenstichting, Gossweiler Foundation, Radboud university medical center, and uniQure, receives royalties from BSL — Springer Nature, and has served on a scientific advisory board of uniQure.
Figures
References
-
- Klockgether T, Mariotti C, Paulson HL. Spinocerebellar ataxia Nat Rev Dis Primers. 2019;5(1):24. - PubMed
-
- Lopez-Bastida J, Perestelo-Perez L, Monton-Alvarez F, Serrano-Aguilar P. Social economic costs and health-related quality of life in patients with degenerative cerebellar ataxia in Spain. Mov Disord. 2008;23(2):212–217. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
