

Impact of Pharmacist-Led Heart Failure Clinic on Optimization of Guideline-Directed Medical Therapy (PHARM-HF)
- PMID: 35501544
- PMCID: PMC9060399
- DOI: 10.1007/s12265-022-10262-9
Impact of Pharmacist-Led Heart Failure Clinic on Optimization of Guideline-Directed Medical Therapy (PHARM-HF)
Abstract
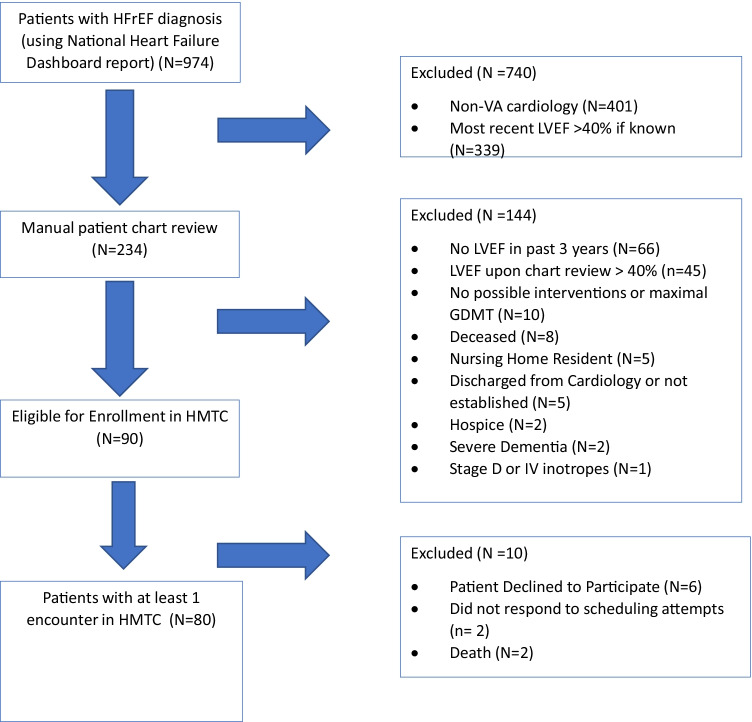
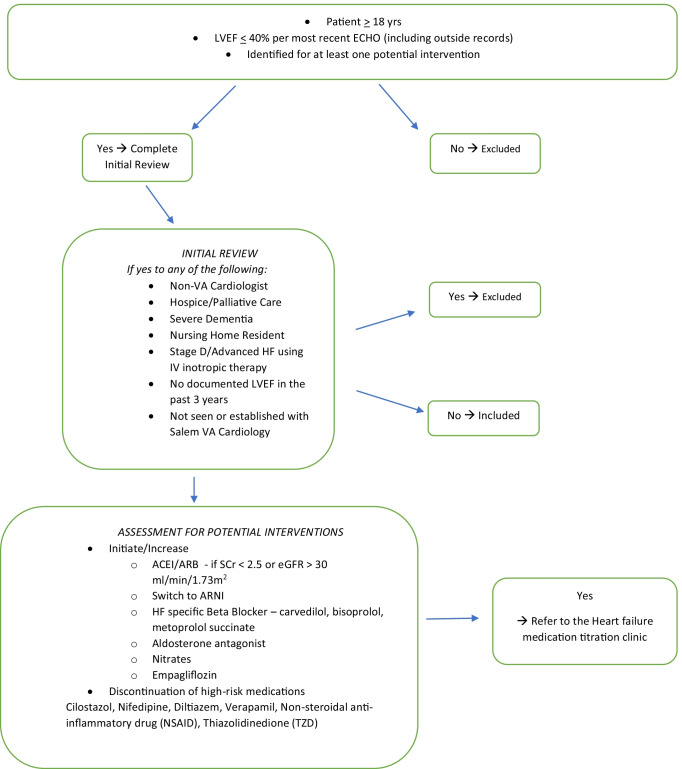
This prospective study included patients with heart failure (HF) with reduced ejection fraction (HFrEF) with LVEF < = 40% to evaluate the impact of pharmacist on guideline directed medical therapy (GDMT). The primary outcome was to compare proportion of triple GDMT achieved for Angiotensin-Converting-Enzyme-Inhibitors (ACEI)/Angiotensin-Receptor-Blockers (ARB)/Angiotensin-Receptor-Neprilysin-Inhibitors (ARNI), beta-blockers, aldosterone antagonists (AA), and quadruple GDMT which in additional to triple therapy, included Sodium glucose co-transporter 2 inhibitor (SGLT2i) at 90-day post-enrollment compared to baseline. Secondary endpoints included achieving target and/or maximally tolerated ACEI/ARB/ARNI and beta-blockers combined and individually as well as SGLT2i and AA GDMT at 90-day post-enrollment compared to baseline. We also compared combined and individual HF-related hospitalization/emergency room (ER) visits 90 days pre-/post-enrollment. Of the total 974 patients screened, 80 patients seen at least once in the heart failure medication titration clinic (HMTC) were included in the analysis. Median (IQR) age was 71 (57-69) years with majority white male. There was a significant improvement in the proportion of patients who achieved quadruple GDMT (p = 0.001) and triple GDMT (p-value = 0.020) at 90-day post-enrollment compared to baseline. The secondary GDMT outcomes were also significantly increased at 90 days post-enrollment compared to baseline. Significant difference in mean as well as proportion of combined HF-related hospitalization/ER-visits was found 90 days pre-/post-enrollment (p = 0.047). Our study found that pharmacist's intervention increased the proportion of patients who achieved GDMT at 90 days.
Keywords: ACE inhibitor; Aldosterone antagonist; B-adrenergic blockers; Congestive heart failure; Guideline-directed medical therapy (GDMT); KCCQ-12; Medication therapy management; Pharmacists; Sodium glucose co-transporter 2 inhibitor; Veterans.
© 2022. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
Tanvi Patil, Salihah Ali, Alamdeep Kaur, Meghan Akridge, Davida Eppes, James Paarlberg, and Amitabh Parashar have nothing to disclose.
Nabil Jarmukli has the following conflict of interest to disclose pertaining to one of the drugs utilized in this study:
2017–2021: Principal Investigator BI Salem VA Medical Center, EMPEROR-Reduced Study
2017–2021: Principal Investigator BI Salem VA Medical Center, EMPEROR-Preserved Study
KCCQ-12 Instrument for Clinical Users was purchased for use during the study duration.
Figures
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, Djousse L, MSV E, Ferguson JF, Fornage M, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, Perak AM, Rosamond WD, Roth GA, UKA S, Satou GM, Schroeder EB, Shah SH, Shay CM, Spartano NL, Stokes A, Tirschwell DL, LB VW, Tsao CW. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2020 update: A report from the American Heart Association. Circulation. 2020;141(9):e139–e596. doi: 10.1161/CIR.0000000000000757. - DOI - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136(6):e137–e161. doi: 10.1161/CIR.0000000000000509. - DOI - PubMed
-
- Maddox TM, Januzzi JL, Jr, Allen LA, Breathett K, Butler J, Davis LL, Fonarow GC, Ibrahim NE, Lindenfeld J, Masoudi FA, Motiwala SR, Oliveros E, Patterson JH, Walsh MN, Wasserman A, Yancy CW, Youmans QR. 2021 Update to the 2017 ACC expert consensus decision pathway for optimization of heart failure treatment: Answers to 10 pivotal issues about heart failure with reduced ejection fraction: A report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2021;77(6):772–810. doi: 10.1016/j.jacc.2020.11.022. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
